

| Journal of Medical Cases, ISSN 1923-4155 print, 1923-4163 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Med Cases and Elmer Press Inc |
| Journal website http://www.journalmc.org |
Case Report
Volume 4, Number 10, October 2013, pages 667-669
Unilateral Agenesis of Pulmonary Artery
Gulfidan Cakmaka, d, Nurdan Gocgunb, Emre Evrenb, Zuhal Aydan Saglamc
aChest Disease, Haseki Training and Research Hospital, Haseki Millet Caddesi, Aksaray-Istanbul, Turkey
bRadiology, Haseki Training and Research Hospital, Haseki Millet Caddesi, Aksaray-Istanbul, Turkey
cFamily Medicine, Haseki Training and Research Hospital; Haseki Millet Caddesi, Aksaray-Istanbul, Turkey
dCorresponding author: Gulfidan Cakmak, Chest Disease, Haseki Training and Research Hospital, Haseki Millet Caddesi, Aksaray-Istanbul, Turkey
Manuscript accepted for publication August 5, 2013
Short title: Unilateral Agenesis of Pulmonary Artery
doi: https://doi.org/10.4021/jmc1428w
| Abstract | ▴Top |
Isolated unilateral absence of pulmonary artery is uncommon. Although not certain, genetic, teratogenic and mechanical factors are held responsible. The anomaly results from the involution of the proximal sixth aortic arch. In this report we present an asymptomatic 24 yrs old male patient. Unilateral right-sided absence of pulmonary artery was diagnosed by thoracic computerized tomography (CT) and angiographic evaluation.
Keywords: Congenital pulmonary disease; Pulmonary artery agenesis; Pulmonary artery disease
| Introduction | ▴Top |
Isolated unilateral agenesis of pulmonary artery was first defined at 1868. Although the exact prevalance is unknown, in a study it is estimated as 1/200,000. Congenital unilateral agenesis of pulmonary artery is a rare anomaly which is frequently associated with other congenital cardiovascular anomalies such as tetralogy of Fallot or septal defects. In 37% of cases left pulmonary artery is absent while in 63% the right one is absent. Nearly 30% of patients are asymptomatic. When symptomatic, patients may experience chest pain, pleural effusion, recurrent pulmonary infections, dyspnea or limited exertion or hemoptysis. Several methods are used in diagnosis such as computerized tomography, bronchography, perfusion scintigraphy, echocardiography and cardiac catheterisation. Massive hemoptysis, cardiac insufficiency, bronchectasis and necrotizing bronchopnemonia may be included among the complications. The following case report presents a patient who was not diagnosed until adult ages.
| Case Report | ▴Top |
A 24-year-old man was admitted to our hospital with dyspnea. He smoked cigarettes 8 pcks/year and currently he was a light smoker. His medical and family history was unremarkable. The physical examination and laboratory findings (biochemical markers, C-reactive protein (CRP), eritrocyt sedimentation rate (ESR)) were normal as well. Respiratory function test revealed slight restriction. Chest x-ray confirmed the right sided shrunken lung and hyperinflation of the left one. 3-D rotational angiography was performed following the thorax CT which revealed atresia of right pulmonary artery. [(MIP) minimum intensity projection images seen Figure 1 and 2, volume rendering (VR) images seen Figure 3 and 4 and Thorax CT angiography image seen Figure 5 of the patient].
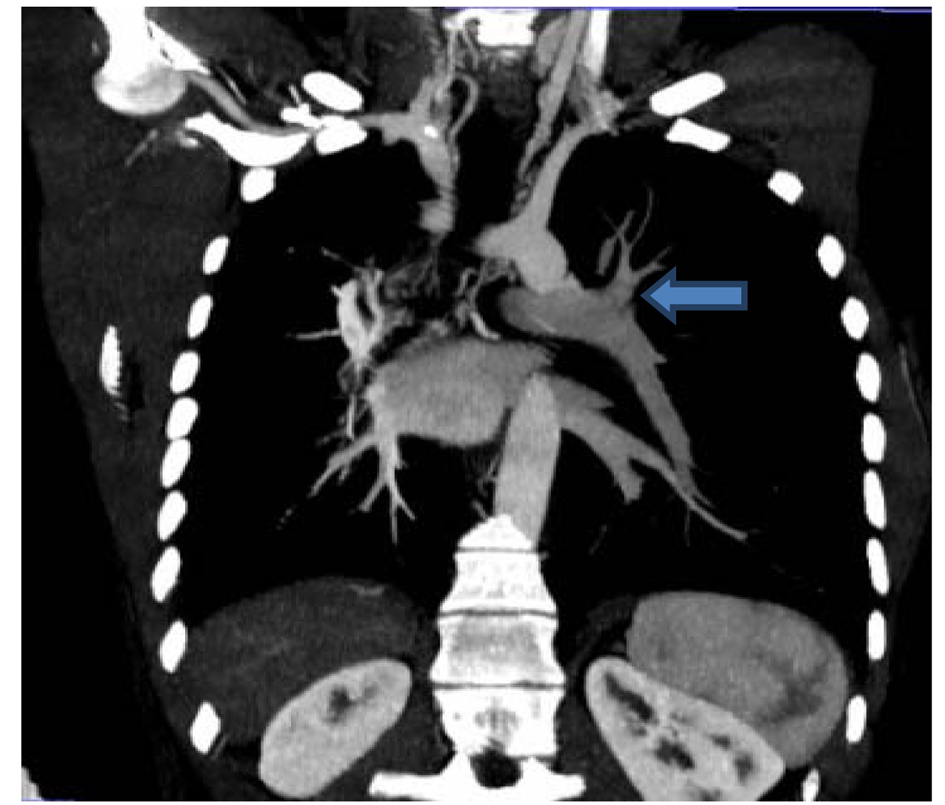 Click for large image | Figure 1. MIP coronal mediasten window. Left arrow: Left pulmonary arter and its branchs; in right absence pulmonary arter. |
 Click for large image | Figure 2. MIP coronal image, lung parenchyma window; right upper and lower arrows: shows the systemic collateral vessels. |
 Click for large image | Figure 3. VR axial image; the right pulmonary artery is atresic. Right arrow shows systemic collateral vessels. |
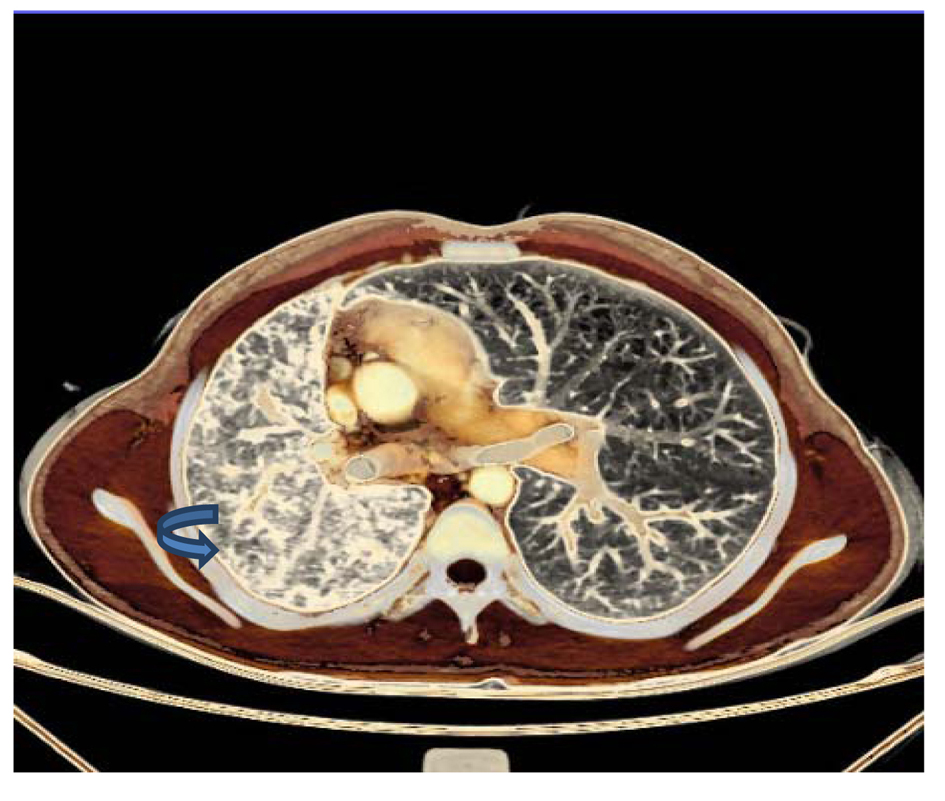 Click for large image | Figure 4. VR image; Volume loss at the right lung with pulmonary atresia compared to the left one; deviation of the mediastinal and bronchial structures to the right and increased interstitial density at the parenchyme. |
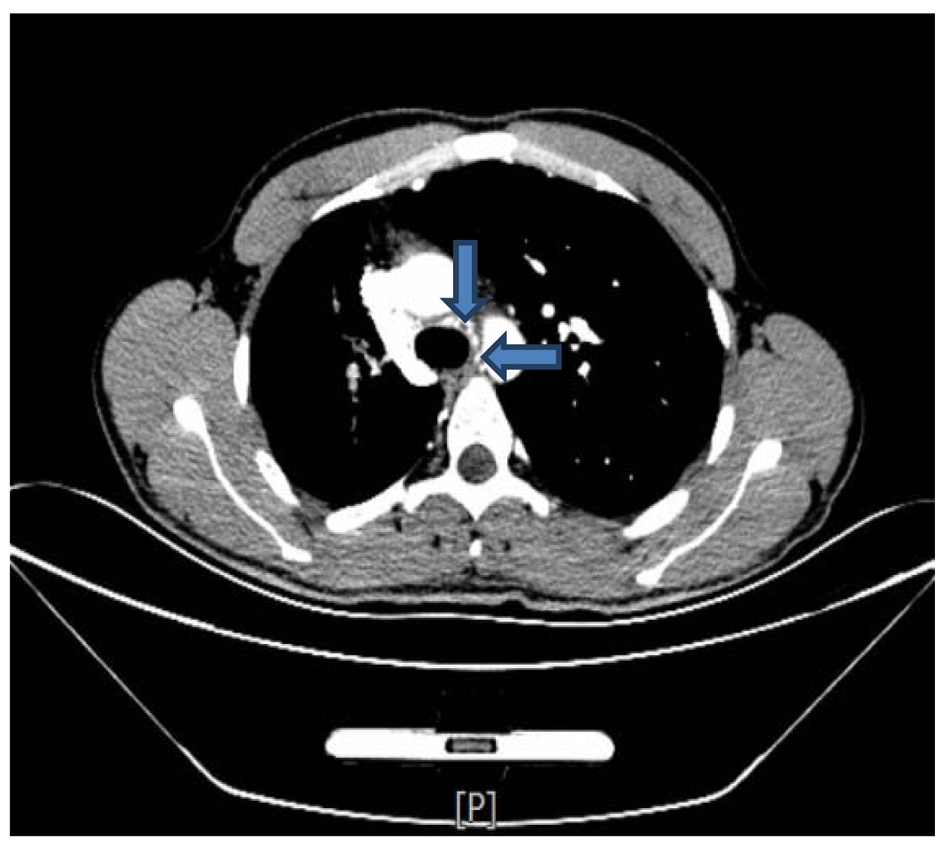 Click for large image | Figure 5. Thorax CT angiography, axial plan, mediastinal window; arrows; systemic collateral vessels surrounding the trachea. |
| Discussion | ▴Top |
Bilateral agenesis of pulmonary artery is incompatible with life [1-6]. Isolated agenesis of pulmonary artery is a rare congenital anomaly [6, 7], 108 cases were reported during the timeframe between 1974 and 2000 [8]. Cardiovascular, gastrointestinal, neuromusculoskeletal and genitourinary system anomalies may coexist in 50% of cases [6]. Symptoms become evident at very early ages in cases in which other congenital anomalies associate. There wasn’t any additional system anomaly in our case. Since this anomaly progresses asymptomatically in adults, the cases are diagnosed by chest radiographs taken incidentally. Contrary to Komatsu, Walter and Gulhan’s cases, our case did not present with hemoptysis [5, 7, 9]. Despite the other cases reported in literature, bronchectasis was not determined in our case although there was a volume loss at the right lung. The absence of coexisting bronchectasis and cardiac or another congenital anomaly is probably the reason for the negative findings in previous health screenings. The prognosis of isolated right pulmonary agenesis is better than the left one and it is less associated with other congenital anomalies [6], 20% of cases of isolated right pulmonary agenesis is associated with pulmonary hypertension. Asymptomatic patients with pulmonary hypertension may become symptomatic at pregnancy or high altitudes [10, 11]. Echocardiographic evaluation of our patient revealed pulmonary systolic hypertension. Since the effected side provides the blood from systemic circulation, the progression of left to right shunt may lead to heart failure in future. CT angiography of our case revealed that the right lung supplied blood from systemic circulation. Nevertheless he hadn’t symptoms of heart failure for the time being.
When asymptomatic, unilateral absence of pulmonary artery presents at incidental chest x-rays with small hilar shadow and hyperlucent lung tissue at the effected side. In our case, posterioanterior chest radiography taken for general examination revealed the absence of a pulmonary arterial veya hilar shadow which was suggestive of a vascular pathology in differential diagnosis. Definitive diagnosis in this type of cases is made by pulmonary arteriography. Eventually, we diagnosed our case by CT angiography. Hyperlucency was determined in most cases presented in literature [6, 7, 12-14]. Unlike the cases with Swyer-James-MacLeod syndrome, in our case, the right main pulmonary artery was not detected at pulmonary CT angiography [12, 13]. The upper right lung was fed by the branches of thyrocervical truncus while the medium and lower lung’s blood supply came from the branches of intercostal arteries. Asymptomatic cases do not require treatment while surgical treatment may be planned for coexisting cardiac anomalies in cases with absence of left pulmonary artery. Pneumonectomy of the affected side may be indicated in case hemoptysis becomes life-threatening or there are cystic bronchectasic formations.
Revascularisation is performed in selected cases [6]. Surgical treatment was not an option in this present case since bronchectasis and cardiac or any other genetic vascular malformation was not determined at the hypoplastic pulmonary tissue [14-17]. Isolated absence of pulmonary artery may not be diagnosed until they reach adulthood because of the asymptomatic benign course or misdiagnosis [8, 18, 19]. The presence of any hilar pathological image at chest roentgenograms taken for any other purpose should suggest vasculary anomalies. In addition, unilateral atresia of pulmonary artery should be regularly followed up closely for progression of possible complications.
Conflict of Interest
There was no conflict of interest among authors.
| References | ▴Top |
- Pool PE, Vogel JH, Blount SG, Jr. Congenital unilateral absence of a pulmonary artery. The importance of flow in pulmonary hypertension. Am J Cardiol. 1962;10:706-732.
doi - Bouros D, Pare P, Panagou P, Tsintiris K, Siafakas N. The varied manifestation of pulmonary artery agenesis in adulthood. Chest. 1995;108(3):670-676.
doi pubmed - Gamba A, Villani M, Tiraboschi R, Annecchino P, Crupi G, Vanini V, Brunelli F, et al. [Surgical treatment of the tetralogy of Fallot with a single pulmonary artery]. G Ital Cardiol. 1984;14(7):499-504.
pubmed - Whitman G, Stephenson LW, Weinberg P. Vascular ring: left cervical aortic arch, right descending aorta, and right ligamentum arteriosum. J Thorac Cardiovasc Surg. 1982;83(2):311-315.
pubmed - de Mello Junior WT, Coutinho Nogueira JR, Santos M, Pelissari Franca WJ. Isolated absence of the right pulmonary artery as a cause of massive hemoptysis. Interact Cardiovasc Thorac Surg. 2008;7(6):1183-1185.
doi pubmed - Sirvanci M, Karaman K, Duran C, Onat L, Ozer K. Unilateral pulmonary agenesis. Turk Gogus Kalp Damar Cer Derg 1999; 7: 6, 486-488 (in Turkish).
- Gulhan M, Simsek Utku E, Akpınar E, Korkmaz S, Bilgic S. Parsiyel pulmoner arter agenezisi olan olguda hemoptizi ve tanisal gecikme. Tuberkuloz ve Toraks Dergisi 2009; 57(2): 223-227 (in Turkish).
- Ten Harkel AD, Blom NA, Ottenkamp J. Isolated unilateral absence of a pulmonary artery: a case report and review of the literature. Chest. 2002;122(4):1471-1477.
doi pubmed - Komatsu Y, Hanaoka M, Ito M, Yasuo M, Urushihata K, Koizumi T, Fujimoto K, et al. Unilateral absence of the pulmonary artery incidentally found after an episode of hemoptysis. Intern Med. 2007;46(21):1805-1808.
doi pubmed - Stiller RJ, Soberman S, Turetsky A, Lockwood C, Haddad R. Agenesis of the pulmonary artery: an unusual cause of dyspnea in pregnancy. Am J Obstet Gynecol. 1988;158(1):172-173.
pubmed - Hackett PH, Creagh CE, Grover RF, Honigman B, Houston CS, Reeves JT, Sophocles AM, et al. High-altitude pulmonary edema in persons without the right pulmonary artery. N Engl J Med. 1980;302(19):1070-1073.
doi pubmed - Ozlu T, Erdinc E. Tek tarafli parlak akciger. TUSAD XIX. Ulusal Kongresi, Sozlu Bildiri. 20-24 Ekim 1991, Bursa: Erol Offset; 1991. s. 228-232(in Turkish).
- Okten F, Dilmac A, Yılmaz F, Calisir HC, Ogretensoy M. Swyer-James Mc Leod sendromu. TUSAD XXIII. Ulusal Kongresi, 11-14 Haziran 1995, Istanbul: Istanbul Universitesi Basimevi; 1995(in Turkish).
- Okutan O, Ugan H, Kaya H, Taş D, Demirer E, Apaydın M, Calıskan T. Izole tek tarafli pulmoner arter yoklugu: Olgu sunumu Isolated unilateral absence of pulmonary artery: a case report. Turk Gogus Kalp Damar Cer Derg 2010;18(1):67-70(in Turkish).
- Atik E, Tanamati C, Kajita L, Barbero-Marcial M. Isolated unilateral pulmonary artery agenesis: evaluation of natural and long term evolution after corrective surgery. Arq Bras Cardiol. 2006;87(4):423-428.
doi pubmed - Karatas Z, Alp H, Altin H, Baysal T. Unilateral pulmonary artery agenesis: clinical and laboratory findings of four cases and diagnostic clues for pediatricians. Anadolu Kardiyol Derg. 2012;12(7):603-605.
pubmed - Oztunc F, Ozkutlu S, Bilgic A, Ozme S, Ozem S. Fallot Tetralojisi ile Birlikte Tek Tarafli Pulmoner Arter Yoklugu ve Anormal Orijinli Pulmoner Arter Vakalari. Turkiye Klinikleri Kardiyoloji. 1990: Cilt 3, Sayi 4, Ekim, 280-283(in Turkish).
- Presbitero P, Bull C, Haworth SG, de Leval MR. Absent or occult pulmonary artery. Br Heart J. 1984;52(2):178-185.
doi pubmed - Perez-Pampin E, Campos-Franco J, Alegria AM, Rigueiro P. Isolated unilateral pulmonary artery agenesis. Intern Med. 2012;51(2):233.
doi pubmed
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Medical Cases is published by Elmer Press Inc.