

| Journal of Medical Cases, ISSN 1923-4155 print, 1923-4163 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Med Cases and Elmer Press Inc |
| Journal website http://www.journalmc.org |
Case Report
Volume 2, Number 2, April 2011, pages 44-47
Successful Treatment of Statin Resistant Hypercholesterolemia by an Inhibitor of Cholesterol Absorption, Ezetimibe
Yoshitaka Maedaa, b, Yuya Arakia, Tomomi Unoa, Keisuke Nishigakia, Naoto Inabaa
aNephrology Division, Department of Internal Medicine, Toride Kyodo General Hospital, 2-1-1 Hongo, Toride, Ibaraki 302-0022, Japan
bCorresponding author: Yoshitaka Maeda
Manuscript accepted for publication January 13, 2011
Short title: Ezetimibe-Responsive Hypercholesterolemia
doi: https://doi.org/10.4021/jmc124w
| Abstract | ▴Top |
HMG-CoA reductase inhibitors (statins) are frequently prescribed against hypercholesterolemia, and these agents successfully suppress levels of serum LDL-cholesterol in most cases. We experienced a case of hypercholesterolemia resistant to statins, but well responsive to an inhibitor of cholesterol absorption in the intestine, ezetimibe. The case was a 58-year-old, non-obese female with persistent high-levels of LDL-cholesterol (LDL-Cho) around 200 (193 - 204) mg/dl even after administration of statins, pitavastatin or rosuvastatin. An inhibitor of cholesterol absorption, ezetimibe was added to rosuvastatin, which resulted in lowering serum LDL-Cho levels to 90 mg/dl. The actual reduction rate of LDL-Cho was 5.4% by rosuvastatin alone, and this rate was up to 53.4% by adding ezetimibe. These results suggest that enhanced cholesterol absorption, rather than cholesterol synthesis, caused hypercholesterolemia in this case. Cholesterol absorption is accelerated in some diseases or conditions, such as diabetes mellitus and obesity, both of which were not identified in this case. Unknown genetic or acquired abnormalities in the intestinal cholesterol-transporting system may be involved in developing hypercholesterolemia. Hence, suppression of cholesterol absorption is a considerable option for hypercholesterolemia resistant to statins.
Keywords: HMG CoA reductase; NPC1L1; Cholestanol
| Introduction | ▴Top |
Hypercholesterolemia, except for familial homozygotes, could be successfully treated in most cases with 3-hydroxyl-3-methylglutaryl coenzyme A (HMG CoA) reductase inhibitors (statins) with substantial effect of lowering serum LDL-cholesterol (LDL-Cho) levels [1] and sufficient tolerability in patients [2]. Clinical problems in administrating statins are restricted to a few cases [3], and some potency of statins in lipid-lowering is generally anticipated.
Ezetimibe [4], an inhibitor of cholesterol absorption, has been available in Japan since 2007. In general, ezetimibe has less effect of lowering serum LDL-Cho levels than those of statins. Therefore, ezetimibe is usually prescribed with statins or fibrates to reduce serum LDL-Cho levels sufficiently in most cases, and is seldom prescribed alone.
We experienced a case of hypercholesterolemia resistant to statins, but well responsive to ezetimibe. Accelerated absorption of cholesterol in the intestine, rather than increased LDL-Cho synthesis, seemed a major cause of hypercholesterolemia in this case.
| Case Report | ▴Top |
The case was a 58-year-old female with hypercholesterolemia that had been repeatedly pointed out by the health check for the past several years. Although the patient had received one of a strong statin, pitavastatin, from an outpatient clinic, serum LDL-cholesterol levels had not been suppressed sufficiently, and stayed above 200 mg/dl. Then the patient visited Toride Kyodo General Hosptial to undergo further examinations for finding out more effective treatments against her hypercholesterolemia. The patient had no past history of any disease other than hypercholesterolemia, which was not found in her family and relatives. The patient counseled dietitians on cholesterol-restriction diet, and any unusual eating habit was not identified. She did not receive any other kinds of drugs and supplements.
The patient was 159 cm tall and weighed 54.4 kg (BMI 21.5). The blood pressure was 96/64 mmHg. Heart sounds were normal and rhythm was regular. The lungs were clear. The bruit was not audible in the neck and the abdomen. Any xanthoma-like lesion was not found in her conjunctiva and ankles.
According to the health check done in September 2009 when the patient did not receive any drugs, serum total cholesterol (T Cho) and LDL-Cholesterol (LDL-Cho) of the patient was 315 and 209 mg/dl, respectively (Fig. 1). On the first visit, serum total cholesterol (T Cho) and LDL-Cholesterol (LDL-Cho) of the patient was 303 and 204 mg/dl, respectively (Table 1). Any other abnormal findings were not noted in the routine blood examination (Table 1). By initiating another strong statin, 2.5 mg/day of rosuvastatin [5], these levels were suppressed to 279 mg/dl in T Cho and 193 mg/dl in LDL-Cho, but these effects seemed unsatisfactory. The drug adherence of the patient was repeatedly ensured during the counseling at the outpatient unit. Since similar ineffectiveness of pitavastatin prescribed before was noted, an inhibitor of cholesterol-absorption, ezetimibe (10 mg daily), was added to losuvastatin. A month later, her serum T Cho was decreased to 167 mg/dl, along with reduction of LDL-Cho to 90 mg/dl. The serum lathosterol, campesterol, sitosterol, and cholestanol were 320, 230, 150, and 360µg/dl, respectively under co-administration of losuvastatin and ezetimibe. Serum cholestanol/cholesterol ratio was 155.2 µg per 100 mg of cholesterol.
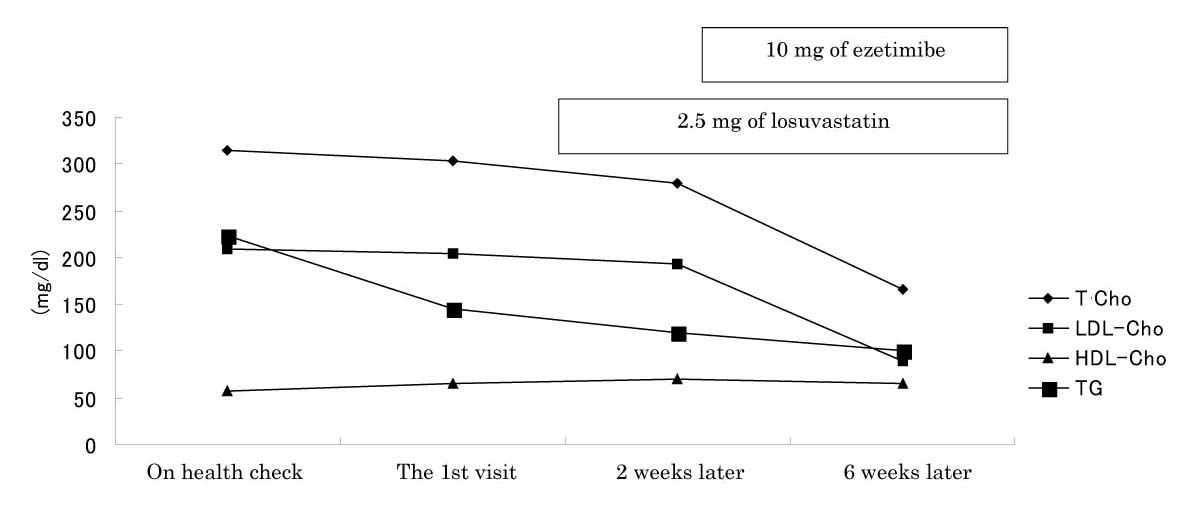 Click for large image | Figure 1. Clinical Course. The reduction rate of LDL-Cho by rosuvastatin was only 5.4 %, and the rate was remarkably increased to 53.4% by adding ezetimibe. |
The right and left ankle-brachial index (ABI) were 1.11 and 1.09. The ultrasonic examination revealed thickening of carotid intima-media thickness (IMT) up to 2.1 mm with plaques.
 Click to view | Table 1. Laboratory Findings |
| Discussion | ▴Top |
Ezetimibe is a new class of lipid-lowering drug that suppress cholesterol absorption in the intestine through the inhibitory effect on the cholesterol transporter, Niemann-Pick C1 Like 1 (NPC1L1) protein [6, 7]. Contrary to adsorbants, ezetimibe has no effect on the absorption of bile acids and liposoluble proteins [4]. The averaged lowering-effect of ezetimibe alone on serum LDL-cholesterol was reported to be around 17.4% [4].
Statin-resistant hypercholesterolemia has been reported to be related to genetic polymorphisms of HMG-CoA reductase [8] and to drug metabolism [9, 10], or in secondary hypercholesterolemia, such as nephrotic syndrome and hypothyroidism [11]. Accelerated cholesterol absorption in the intestine may reduce lipid-lowering effect of statins in type 2 diabetes mellitus [12] since the serum cholesterol levels were partially affected by cholesterol absorption [13]. However, any known diseases or conditions related to increased cholesterol absorption were not identified in this case. Remarked effect of ezetimibe on serum cholesterol in this case suggested that accelerated cholesterol absorption, rather than increased cholesterol synthesis, subsequently elevated serum LDL-cholesterol levels. Since the amount of cholesterol absorption is regulated by the balance of excretion through ATP-binding cassette hetero-dimeric transportes G5/G8 (ABCG5/G8) and absorption through NPC1L1, genetic polymorphisms of either ABCG5/G8 or NPC1L1 affect serum LDL-Cho levels [14, 15], responses to ezetimibe [16-18], absorption of plant sterols [19, 20], and a consequent risk for coronary heart disease [14]. This case might have such a genetic variance or an acquired abnormality that would be identified in the future.
Cholestanol is a metabolite of cholesterol, produced by bacteria in the gut, absorbed in the intestine and never metabolized until the excretion into feces. Hence, the cholestanol/cholesterol ratio was reported to reflect the level of cholesterol absorption [21, 22], although the averaged range has not been established. According to the report by Strandlberg TE, in 376 of home-dwelling individuals aged 75 years and older with cardiovascular diseases (M/F: 129/247), absolute mean serum cholestanol concentration was 313.3 ± 100.2 µg/dl, and the mean concentration relative to 100 mg of serum cholesterol was 156.7 ± 40.5 µg [21]. In the same study, the mean concentrations of the plant sterols, lathosterol, sitosterol, and campesterol were 142.2, 111.2, 223.0µg/100 mg cholesterol in the alive group, and 130.9, 128.3, 245.5 µg/100 mg cholesterol respectively in the dead group [21]. The case in this report showed the similar levels of cholestanol and the plant sterols under the suppression of cholesterol-absorption by ezetimibe, which might suggest rather accelerated cholesterol and cholestanol absorption before ezetimibe had been administered.
In conclusion, the case reported here did not have any conditions or diseases that has been reported to accelerate cholesterol absorption; hence, any genetic or acquired abnormality of either ABCG5/G8 or NPC1L1 might be involved in hypercholesterolemia. Further study is needed to identify the actual mechanism of hypercholesterolemia in this case.
| References | ▴Top |
- Dembowski E, Davidson MH. A review of lipid management in primary and secondary prevention. J Cardiopulm Rehabil Prev 2009;29(1):2-12.
pubmed - Brown WV. Safety of statins. Curr Opin Lipidol 2008;19(6):558-562.
pubmed doi - Devroey D, Betz W, Coigniez P, Lauwers R, Velkeniers B. A "bad responder" to statins. Cardiology 2002;97(4):230-232.
pubmed doi - Keller U: A new class of lipid-lowering drugs. Ezetimibe. Heart Drug 2003; 3:214-216.
- Gandhi SK, Jarbrink K, Fox KM, Brandrup-Wognsen G. Effectiveness of rosuvastatin in reducing LDL-C and target LDL-C goal attainment in real-world clinical practice. Curr Med Res Opin 2009;25(12):2817-2828.
pubmed doi - Altmann SW, Davis HR, Jr., Zhu LJ, Yao X, Hoos LM, Tetzloff G, Iyer SP, et al. Niemann-Pick C1 Like 1 protein is critical for intestinal cholesterol absorption. Science 2004;303(5661):1201-1204.
pubmed doi - Turley SD. The role of Niemann-Pick C1 - Like 1 (NPC1L1) in intestinal sterol absorption. J Clin Lipidol 2008;2(2):S20-S28.
pubmed doi - Peters BJ, Klungel OH, de Boer A, Maitland-van der Zee AH. Genetic determinants of response to statins. Expert Rev Cardiovasc Ther 2009;7(8):977-983.
pubmed doi - Tachibana-Iimori R, Tabara Y, Kusuhara H, Kohara K, Kawamoto R, Nakura J, Tokunaga K, et al. Effect of genetic polymorphism of OATP-C (SLCO1B1) on lipid-lowering response to HMG-CoA reductase inhibitors. Drug Metab Pharmacokinet 2004;19(5):375-380.
pubmed doi - Romaine SP, Bailey KM, Hall AS, Balmforth AJ. The influence of SLCO1B1 (OATP1B1) gene polymorphisms on response to statin therapy. Pharmacogenomics J 2010;10(1):1-11.
pubmed doi - Krieger EV, Knopp RH. Hypothyroidism misdiagnosed as statin intolerance. Ann Intern Med 2009;151(1):72.
pubmed - Lally S, Tan CY, Owens D, Tomkin GH. Messenger RNA levels of genes involved in dysregulation of postprandial lipoproteins in type 2 diabetes: the role of Niemann-Pick C1-like 1, ATP-binding cassette, transporters G5 and G8, and of microsomal triglyceride transfer protein. Diabetologia 2006;49(5):1008-1016.
pubmed doi - Kesaniemi YA, Miettinen TA. Cholesterol absorption efficiency regulates plasma cholesterol level in the Finnish population. Eur J Clin Invest 1987;17(5):391-395.
pubmed doi - Polisecki E, Peter I, Simon JS, Hegele RA, Robertson M, Ford I, Shepherd J, et al. Genetic variation at the NPC1L1 gene locus, plasma lipoproteins, and heart disease risk in the elderly. J Lipid Res 2010;51(5):1201-1207.
pubmed doi - Chen CW, Hwang JJ, Tsai CT, Su YN, Hsueh CH, Shen MJ, Lai LP. The g.-762T>C polymorphism of the NPC1L1 gene is common in Chinese and contributes to a higher promoter activity and higher serum cholesterol levels. J Hum Genet 2009;54(4):242-247.
pubmed doi - Simon JS, Karnoub MC, Devlin DJ, Arreaza MG, Qiu P, Monks SA, Severino ME, et al. Sequence variation in NPC1L1 and association with improved LDL-cholesterol lowering in response to ezetimibe treatment. Genomics 2005;86(6):648-656.
pubmed doi - Hegele RA, Guy J, Ban MR, Wang J. NPC1L1 haplotype is associated with inter-individual variation in plasma low-density lipoprotein response to ezetimibe. Lipids Health Dis 2005;4:16.
pubmed - Wang J, Williams CM, Hegele RA. Compound heterozygosity for two non-synonymous polymorphisms in NPC1L1 in a non-responder to ezetimibe. Clin Genet 2005;67(2):175-177.
pubmed doi - Zhao HL, Houweling AH, Vanstone CA, Jew S, Trautwein EA, Duchateau GS, Jones PJ. Genetic variation in ABC G5/G8 and NPC1L1 impact cholesterol response to plant sterols in hypercholesterolemic men. Lipids 2008;43(12):1155-1164.
pubmed doi - Rudkowska I, AbuMweis SS, Nicolle C, Jones PJ. Association between non-responsiveness to plant sterol intervention and polymorphisms in cholesterol metabolism genes: a case-control study. Appl Physiol Nutr Metab 2008;33(4):728-734.
pubmed doi - Strandberg TE, Tilvis RS, Pitkala KH, Miettinen TA. Cholesterol and glucose metabolism and recurrent cardiovascular events among the elderly: a prospective study. J Am Coll Cardiol 2006;48(4):708-714.
pubmed doi - Matthan NR, Lichtenstein AH. Approaches to measuring cholesterol absorption in humans. Atherosclerosis 2004;174(2):197-205.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Medical Cases is published by Elmer Press Inc.