

| Journal of Medical Cases, ISSN 1923-4155 print, 1923-4163 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Med Cases and Elmer Press Inc |
| Journal website http://www.journalmc.org |
Case Report
Volume 11, Number 2, February 2020, pages 41-43
Percutaneous Coronary Intervention in an Octogenarian With Anomalous Origin Arising From Right Sinus: A Rare Case Report
Yeriswamy Mogalahally Channabasappaa, Natraj Setty Hulliurudurga Srinivasa Settya, b, Sandeep Shankara, Ravindranath Kandenahalli Shankrappaa, Jayashree Khargea, Raghu Tagatagere Ramegowdaa, Rahul Patila, Sathish Kerura, Manjunath Cholenahally Nanjappaa
aSri Jayadeva Institute of Cardiovascular Sciences and Research, Bangalore, Karnataka, India
bCorresponding Author: Natraj Setty Hulliurudurga Srinivasa Setty, Sri Jayadeva Institute of Cardiovascular Sciences and Research, Bangalore, Karnataka 560069, India
Manuscript submitted January 29, 2020, accepted February 3, 2020
Short title: PCR for Anomalous Coronary Artery Origins
doi: https://doi.org/10.14740/jmc3429
| Abstract | ▴Top |
Anomalous coronary artery origins are not common in routine clinical practice. The incidence of coronary anomalies in patients undergoing coronary angiography is less than 1%. The greatest challenges faced in the management are delays in identification and difficulty engaging the anomalous coronary artery. Operator experience in promptly identifying the anomaly and selection of the appropriate catheter is critical for successful intervention. We are presenting a case of acute inferior and posterior wall myocardial infarction (MI) with an anomalous origin of the left circumflex artery from the right coronary sinus. Learning objective is that percutaneous coronary intervention (PCI) in an anomalous left circumflex can be technically difficult because selective cannulation of the vessel may not be easy. An anomalous left circumflex artery has a rare presentation of ST-elevation myocardial infarction (STEMI). Complicated STEMI with cardiogenic shock is not commonly seen in anomalous coronary artery origin from the right sinus. Percutaneous intervention in patients with STEMI with an anomalous left circumflex artery has a high risk and is technically challenging.
Keywords: Anomalous coronary artery; Percutaneous coronary intervention; Left circumflex
| Introduction | ▴Top |
Coronary anomalies are a group of congenital disorders with highly variable pathophysiological mechanisms and manifestations [1]. Most of the coronary anomalies are asymptomatic and benign but may cause acute coronary syndrome and sudden cardiac death [2]. Most coronary anomalies are found incidentally during coronary angiography, and 0.6% to 1.55% of patients with coronary artery anomalies are found [3]. Anomalous origin of the circumflex branch from the right coronary artery (RCA) is a rare congenital anomaly. We present a case of an 80-year-old man who has presented to the emergency department with acute inferior and posterior myocardial infarction (MI) with cardiogenic shock. The coronary angiography reveals a left circumflex coronary artery arising from the right sinus, and the patient underwent successful percutaneous coronary intervention (PCI) in the anomalous left circumflex coronary artery.
| Case Report | ▴Top |
An 80-year-old man presented with a history of diabetes mellitus and hypertension for 10 years, and retrosternal chest pain and sweating of 2-h duration. On physical examination, the patient was seen to be anxious, and his heart rhythm was regular with a rate of 90 beats per minute; the blood pressure was 80/60 mm Hg. Cardiac auscultation revealed a left ventricular fourth heart sound. The routine investigation was normal. Venereal Disease Research Laboratory (VDRL), HIV, connective tissue profile, and complete hemogram were normal. Serum biomarkers were elevated (troponin T, troponin I, and creatine kinase-MB). Echocardiography revealed hypokinesia in left circumflex artery (LCX) territory with an ejection fraction of 45%. Electrocardiogram revealed normal sinus rhythm with first-degree atrioventricular (AV) block, ST-elevation in II, III, and aVF limb, and posterior (V7 - V9) chest leads with recurrent ventricular tachycardia (VT) (Fig. 1a-c). The patient was connected to the intra-aortic balloon pump (IABP). After proper consent, we planned for primary PCI through the femoral route. He has preloaded with ticagrelor 180 mg, aspirin 300 mg, and atorvastatin 80 mg. The 6 F Judkins right 3.5 (JR3.5) and Judkins left 3.5 (JL3.5) diagnostic catheters were used for catheterization after administering 1,500 U of heparin. The angiogram of the left system showed no flow-limiting lesion in left anterior descending artery (LAD), and the LCX was not visualized (Fig. 2a). The RCA was a small caliber non-dominant vessel. On gradual pullback of the JR diagnostic catheter, LCX was seen arising from the right sinus showing total proximal thrombotic occlusion (Fig. 2b). The decision was then made to open up the occluded anomalous LCX vessel. An additional 6,000 U heparin was given. Initially, to cannulate the LCX vessel 6F JR guiding catheter, but not to cannulate the LCX, we used AMPLATZER AR catheter and hockey stick catheter subsequently. Because of difficulty in cannulation and lack of adequate support with these catheters, we used a multi-purpose guiding catheter to cannulate anomalous LCX. To cross the lesion, we used 0.014 floppy wire. A 2.5 × 10 mm Sprinter balloon was used at 10 - 14 atm for pre-dilation after dottering the LCX vessel. At 11 atm, a 3.5 × 24 mm drug-eluting stent (DES) was then deployed (Fig. 2c). With a 3.5 × 10 mm NC balloon at 12 - 14 atm post dilation was done. Post stent deployment, there was good opacification of contrast with TIMI III flow in anomalous LCX vessel (Fig. 2d). After the procedure, the patient was hemodynamically stable and was discharged after 2 days.
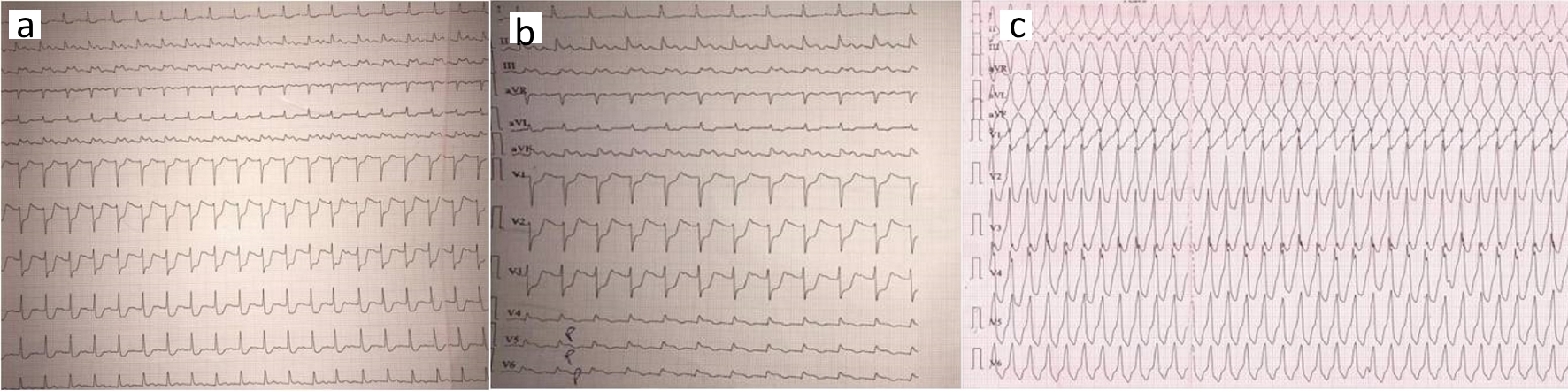 Click for large image | Figure 1. (a) Electrocardiogram showing normal sinus rhythm with first degree AV block, ST-segment elevation in II, III, and aVF; (b) Electrocardiogram showing ST-segment elevation in posterior leads V7 - V9; (c) Electrocardiogram showing recurrent monomorphic VT. AV: atrioventricular; VT: ventricular tachycardia. |
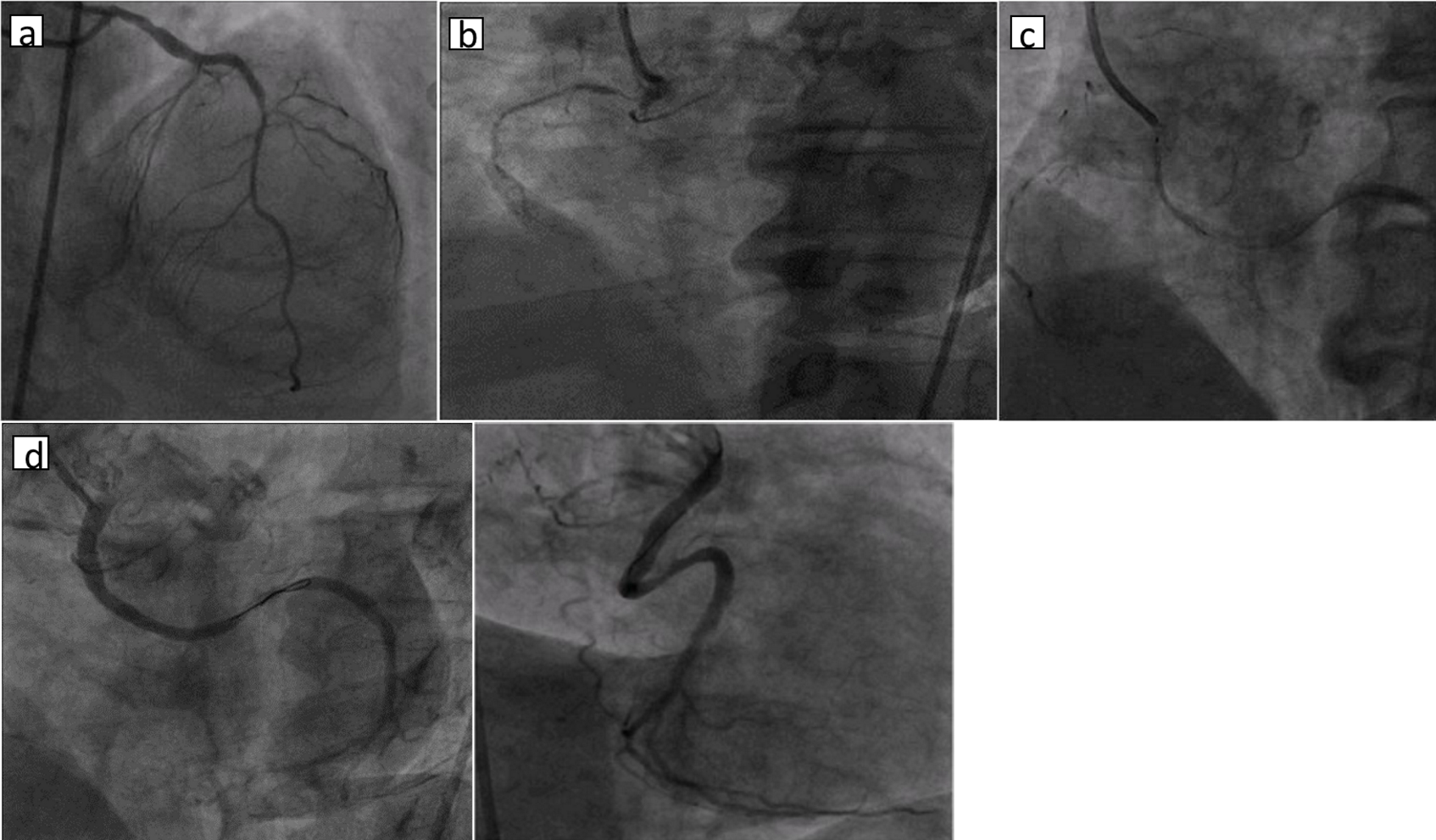 Click for large image | Figure 2. (a) Left coronary angiography showing normal LMCA and LAD; (b) right coronary angiography showing anamalous LCX from right sinus with total occlusion and non-dominant RCA; (c) right coronary angiography showing 3.5 × 24 mm DES deployed at 11 atm; (d) right coronary angiography showing dominant LCX with TIMI III flow (LAO and RAO views). LMCA: left main coronary artery; LAD: left anterior descending artery; LCX: left circumflex artery; DES: drug-eluting stent; LAO: left anterior oblique; RAO: right anterior oblique. |
| Discussion | ▴Top |
The anomalous origin of the left circumflex coronary artery is one of the most frequent anatomic variations [4]. Aberrant LCX, arising from the right coronary sinus, does not predispose the LCX to a higher frequency of obstructive disease. However, in the presence of a significant lesion of LCX, it is essential to recognize the anomaly angiographically and manage it properly [5]. Our patient was a candidate for angioplasty of LCX. PCI of aberrant coronary arteries is challenging technically due to insufficient visualization during coronary angiography, inability to achieve a coaxial engagement of catheter during PCI, the necessity of significant curve in the guidewire and trouble with the advancement of the balloon or the stent delivery system.
Moreover, selecting a suitable guiding catheter is crucial in the performance of angioplasty in the anomalous coronary artery [6]. In our patient initially, we used Judkins catheters to perform angiography. However, during percutaneous transluminal coronary angioplasty (PTCA) of the LCX, cannulation was not possible with the Judkins and Amplatz catheters. The ostium of the LCX was anterior and inferior, and the use of the multi-purpose guiding catheter in this patient provided easy cannulation with enough backup support to ensure proper angiographic opacification. Based on its shape, a large area of support, and location of the artery, we chose a multi-purpose guiding catheter. It provided the maximum stable support required for the smooth passage of the balloon as well as a stent. The tip of the catheter hooked anomalous vessels, and the curve rested stably against the opposite aortic wall. Thus, it appears that the multi-purpose guiding catheter may be the best choice for PTCA of a coronary artery with a similar anomaly.
Conclusions
Prompt identification and engagement of the anomalous artery are the biggest hurdles to the operator in the management of coronary interventions. The selection of appropriate guiding catheters is an important step in the PCI procedure in preventing significant delays. When combined with operator experience, PCI offers a safe therapeutic option for the treatment of anomalous coronary arteries.
Acknowledgments
None to declare.
Financial Disclosure
None to declare.
Conflict of Interest
None to declare.
Informed Consent
The informed consent was obtained.
Author Contributions
YMC contributed to data analysis and study design; NSHSS wrote the paper; SS, RKS, and RTR contributed to data analysis; SK contributed to data collection; JK and RP were involved in reference collection; and MCN gave the final approval.
Abbreviations
LAD: left anterior descending artery; LCX: left circumflex; PCI: percutaneous coronary intervention; STEMI: ST-elevation myocardial infarction; IABP: intra-aortic balloon pump; RCA: right coronary artery; PTCA: percutaneous transluminal coronary angioplasty; MI: myocardial infarction; AV: atrioventricular; VT: ventricular tachycardia; JR: Judkins right; JL: Judkins left; DES: drug-eluting stent
| References | ▴Top |
- Carvalho JS, Silva CM, Rigby ML, Shinebourne EA. Angiographic diagnosis of anomalous coronary artery in tetralogy of Fallot. Br Heart J. 1993;70(1):75-78.
doi pubmed - Bayat P, Masoud F, Ghanbari A, Ganji Harsini S. Anomalous origin of the circumflex branch from the right coronary artery. Int J Morphol. 2013;31(1):169-1.
doi - Aydin M, Ozeren A, Peksoy I, Cabuk M, Bilge M, Dursun A, Elbey MA. Myocardial Ischemia caused by a coronary anomaly: left circumflex coronary artery arising from right sinus of Valsalva. Tex Heart Inst J. 2004;31(3):273-275.
- Verma PK, Bisht DS. Anomalous origin of left main coronary artery from right sinus of Valsalva, a case report. Angiol. 2015;3:160.
- Karadeniz M. Anomalous circumflex coronary artery from right coronary sinus with acute inferior myocardial infarction. Am J Cardiol. 2018;121(suppl 8):e75-e76.
doi - Sarkar K, Sharma SK, Kini AS. Catheter selection for coronary angiography and intervention in anomalous right coronary arteries. J Interv Cardiol. 2009;22(3):234-239.
doi pubmed
This article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Medical Cases is published by Elmer Press Inc.