

| Journal of Medical Cases, ISSN 1923-4155 print, 1923-4163 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Med Cases and Elmer Press Inc |
| Journal website http://www.journalmc.org |
Case Report
Volume 11, Number 2, February 2020, pages 37-40
Takayasu Arteritis Mistaken for Epilepsy: A Case Presenting With Convulsive Syncope
Pedro Pallangyoa, b, e, Nsajigwa Misidaia, Naairah R. Hemeda, Happiness J. Swaia, Zabella Mkojeraa, Smita Bhaliab, Frederick Lyimoc, Jalack Millingad, Salma A. Wibonelad, Mohamed Janabib
aDepartment of Research & Training, Jakaya Kikwete Cardiac Institute, PO Box 65141, Dar es Salaam, Tanzania
bDepartment of Cardiology, Jakaya Kikwete Cardiac Institute, PO Box 65141, Dar es Salaam, Tanzania
cDepartment of Radiology, Muhimbili National Hospital, PO Box 65000, Dar es Salaam, Tanzania
dDepartment of Nursing, Jakaya Kikwete Cardiac Institute, PO Box 65141, Dar es Salaam, Tanzania
eCorresponding Author: Pedro Pallangyo, Department of Research & Training, Jakaya Kikwete Cardiac Institute, PO Box 65141, Dar es Salaam, Tanzania
Manuscript submitted January 23, 2020, accepted February 3, 2020
Short title: Takayasu Arteritis Mistaken for Epilepsy
doi: https://doi.org/10.14740/jmc3424
| Abstract | ▴Top |
Takayasu arteritis (TA) is a chronic inflammatory disease characterized by granulomatous vasculitis that predominantly manifests as panaortitis. This occlusive thromboaortopathy lacks pathognomonic features often resulting in a diagnostic dilemma leading to its under-recognition, misdiagnosis and delayed management. Although neurological manifestations are not uncommon in TA, convulsive syncope as an initial clinical presentation is extremely rare. We report a case of convulsive syncope as a manifesting symptom of TA. A 17-year-old male patient of African origin was referred to us from an upcountry regional hospital with a diagnosis of medically intractable epilepsy for cardiovascular review. He presented with a 28-week history of generalized tonic-clonic seizures followed by loss of consciousness. He denied history of recurrent headaches, fever, visual disturbances, arthralgias, claudication or unintentional weight loss. Physical examination revealed feeble left-sided brachial and radial pulses, elevated blood pressure, differences in blood pressure between arms and left-sided carotid and vertebral bruits. Computed tomography angiogram of his thoracic and abdominal aorta revealed changes suggestive of a diffuse arteritis. Additionally, magnetic resonance angiogram of the brain revealed total occlusion of the left common carotid, left internal carotid, left external carotid and left vertebral arteries. Based on the physical examination and radiological findings, we reached a diagnosis of TA. He was prescribed dexamethasone, methotrexate, acetylsalicylic acid and amlodipine. He had a remarkable recovery and was seizure-free for the last 5 months after discharge. TA may manifest with convulsive syncope mimicking epilepsy. Despite its rarity, presentations of this nature continue to challenge clinicians resulting in delayed diagnosis with irreversible life-threatening consequences to patients. In view of this, physicians should strive to take detailed history and perform thorough physical examination so as to timely pick the characteristic signs of TA especially in patients presenting with unanticipated symptoms.
Keywords: Takayasu arteritis; Occlusive thromboaortopathy; Granulomatous panarteritis; Chronic granulomatous vasculitis; Large vessel vasculitis; Pulseless disease; Convulsive syncope; Takayasu mimicking epilepsy
| Introduction | ▴Top |
Takayasu arteritis (TA) is a chronic inflammatory disease characterized by granulomatous vasculitis that predominantly manifests as panaortitis [1-4]. This occlusive thromboaortopathy has an estimated incidence of two cases/1,000,000 population/year and is more prevalent in Africa, Southeast Asia, and Central and South America [1-4]. The etiology of TA remains poorly understood and likewise its exact pathogenic sequence is yet to be established [1-4]. The disease demonstrates a striking female predilection and commonly but not exclusively presents in the second or third decade of life [1, 3]. Owing to the paucity of distinctive symptoms and absence of a reliable serological marker of disease course, TA often poses a diagnostic dilemma leading to its under-recognition, misdiagnosis and delayed management [1-3].
The hallmark of TA is the granulomatous inflammation that commences from the adventitia and progresses to the intima with resultant segmental stenosis, occlusion, dilatation and aneurysm formation leading to end-organ ischemia [5]. The characteristic proximal arterial involvement usually leaves the brain parenchyma until later stage of disease progression [5]. Takayasu-induced cerebral ischemia may result in a myriad of neurological manifestations including headache, organic confusion, dementia, seizure, meningitis, encephalitis, stroke, visual disturbances and syncope [4-6]. Although between 42% and 80% of patients with TA present with central nervous system (CNS) manifestations, convulsive syncope as the primary presentation is rare [5]. We report a case of convulsive syncope as an initial presentation of TA in a 17-year-old male patient of African origin.
| Case Report | ▴Top |
A 17-year-old male patient secondary student of African origin was referred to us from an upcountry regional hospital with a diagnosis of medically intractable epilepsy for cardiovascular review. He presented with a 28-week history of recurrent convulsive syncope attacks which were unresponsive to anti-epileptic drugs. The seizures were generalized tonic-clonic in nature followed by loss of consciousness of variable duration (10 - 30 min). These episodes were often associated with abrupt change of posture particularly sitting upright and on standing. On average he experienced 1 - 3 episodes daily. He denied bladder/bowel incontinence or presence of aura symptoms following or preceding the convulsive episodes respectively. Neurologist’s notes revealed post-ictal drowsiness with a transient memory impairment following the attack. There was a negative history of recurrent headaches, fever, visual disturbances, arthralgias, claudication or unintentional weight loss. His past medical history was unremarkable and he denied substance abuse.
On examination, he was alert, oriented and well-kempt. He was pale (conjuctival and palmar) but not jaundiced. Oral examination revealed a lateral tongue bite mark with adequate dentition. His left-sided brachial and radial arterial pulses were feeble, whereas pulses on his right side and in both lower limbs were normal. Left-sided carotid and vertebral bruits were noted. His blood pressure (BP) was 169/91 mm Hg on his left and 124/82 mm Hg on the right side. He had a pulse rate of 119 beats/min which was regular and of good volume. He was afebrile (37.2 °C) and had a healthy weight (body mass index (BMI) 21.9 kg/m2). Abdominal examination was uneventful with no evidence of renal bruits or aneurysms. The rest of systemic examination was unremarkable.
His hematological, biochemical, serological and autoimmune tests revealed normal findings except for raised inflammatory markers, i.e. erythrocyte segmentation rate (ESR) 58 mm/h and C-reactive protein (CRP) 27.6 mg/L. A tuberculin test was negative. Echocardiographic examination revealed normal findings except for a trace aortic regurgitation. Due to a clinical suspicion of TA, we ordered a carotid Doppler ultrasound scan (USS) which showed a complete occlusion of the left common, internal and external carotid arteries. On the other hand, renal Doppler USS revealed bilaterally patent vessels with a spontaneous phasic flow. Moreover, both common and deep femoral arteries exhibited a normal course and calibre with no evidence of intraluminal plaque or stenosis on femoral Doppler USS.
Computed tomography (CT) of brain was negative for stroke or space occupying lesions and electroencephalogram (EEG) ruled out likelihood of a focal cerebral pathology. Furthermore, CT angiogram of his thoracic and abdominal aorta revealed changes suggestive of a diffuse arteritis, i.e. irregular narrowing with variable degrees of stenosis, tapering and corrugated appearance (Fig. 1). Additionally, left common carotid, left internal carotid, left external carotid and left vertebral arteries could not be visualized on the magnetic resonance angiogram (MRA) of the brain (Fig. 2).
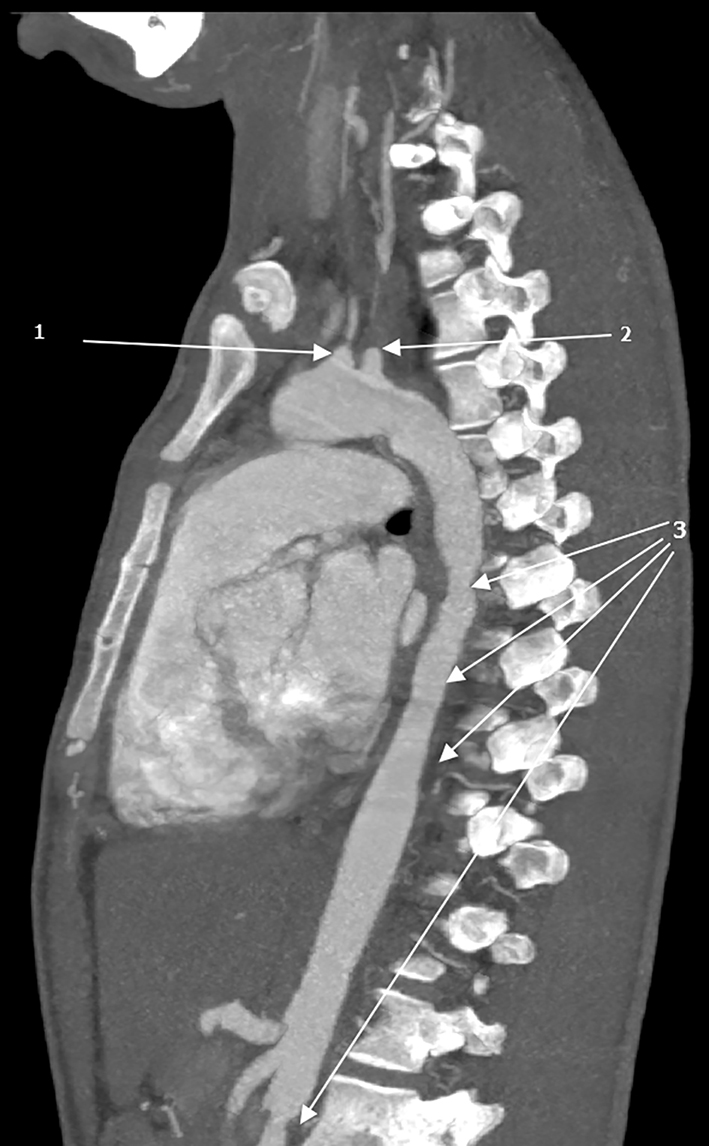 Click for large image | Figure 1. Computed tomography angiogram of thoracic and abdominal aorta displaying (1) left common carotid artery, (2) origin of left subclavian artery and (3) features suggestive of diffuse arteritis, i.e. irregular narrowing with variable degrees of stenosis, tapering and corrugated appearance. |
 Click for large image | Figure 2. Brain magnetic resonance angiogram showing total occlusion of the left common carotid, left internal carotid, left external carotid and left vertebral arteries. |
Based on the clinical presentation and radiological features, our case fulfilled the American College of Rheumatology criteria [7] for TA. He was counseled and dexamethasone (60 mg per day), methotrexate (10 mg per day), acetylsalicylic acid (75 mg once daily) and amlodipine (10 mg once daily) were initiated on the sixth day of hospitalization. The patient had a total of 14 convulsive syncope episodes in the initial 6 days of hospitalization (i.e. before initiation of steroids) and five episodes in the last 7 days. He was discharged home after 13 days of hospitalization in a considerably stable state. We reviewed him as an out-patient at 3 and 6 months. He had a controlled BP (132/78 mm Hg left-sided and 117/71 mm Hg right-sided) and was seizure-free for the last 5 months (i.e. had two episodes within the first month after discharge).
| Discussion | ▴Top |
TA is a rare yet the most common large-vessel vasculitis with an unidentifiable cause and undetermined pathogenesis [1-4]. Owing to the involved vascular territory and the degree of disease progression, TA patients vary greatly in their clinical presentation which is collectively characterized by active and quiescent phases [1-3]. Such unpredictability in its presentation and course often makes the diagnosis of this potentially life-threatening condition difficult and late [1-4].
In spite of their relatively late onset, neurological manifestations are not uncommon in TA [4]. Decreased blood flow resulting from steno-occlusive lesions and/or shifting of the blood flow (steal) is responsible for various TA-associated CNS manifestations [4]. Whereas convulsive syncope as an initial clinical presentation is extremely uncommon [8-12], several other neurological manifestations including headache, vertigo, organic confusion, dementia, meningitis, encephalitis, stroke, visual disturbances and intracranial aneurysms have been commonly associated with TA [4, 6].
As presented in this case, the young boy presented with convulsive syncope which was labelled epilepsy and he was prescribed several anti-seizure drugs with no relief. Due to the absence of other clinical manifestations, it took literally 7 months to reach the definitive diagnosis of TA. Despite all the existing challenges attributable to TA diagnosis, we believe that this case is a clear reminder of how fundamental thorough history taking and physical examination are. We are convinced that despite the rare symptomatology, a couple of TA signs including elevated BP, BP discrepancy between arms, unequal pulses and bruits along the neck region were present but missed during the 7 months course of this case illness.
Worth noting is that, a number of medical conditions may present with generalized tonic-clonic seizures, therefore, not every seizure is epilepsy. Unfortunately, we are living in a world where clinicians have lost clinical examination capabilities and rely almost entirely on laboratory and radiological tests to reach a diagnosis [13-15]. As a result, this form of substitution in clinical discipline has led to increased incorrect diagnoses and a more pricey management approach [15]. Nonetheless, it is imperative for clinicians to be aware of the unusual presentations of TA because a timely and appropriate intervention has the potential to halt the inflammatory process and improve the health-related quality of life.
Despite its rarity, TA may manifest with convulsive syncope mimicking epilepsy. It is necessary for clinicians to understand the dynamic symptomatology of this condition for an early diagnosis and timely management to curb damage accrual and attributable morbidity. Moreover, physicians should strive to take detailed history and perform thorough physical examination so as to timely pick characteristic signs of TA especially in patients presenting with unanticipated symptoms.
Acknowledgments
The authors are grateful to the staff of the Jakaya Kikwete Cardiac Institute for their tireless efforts in daily patient care.
Financial Disclosure
None to declare.
Conflict of Interest
The authors declare that they have no conflict of interest.
Informed Consent
Written informed consent was obtained from the patient’s next of kin for publication of this case report and any accompanying images.
Author Contributions
SB and PP took the history and performed the physical examination. FL interpreted the radiological investigations. JM, HJS, NRH, NM, ZM, SB, SAW and MJ participated in clinical management and counseling of the patient during hospitalization. PP wrote the initial draft of the manuscript. All authors reviewed and contributed to the final version of this case report.
Data Availability
The authors declare that data supporting the findings of this study are available within the article.
Abbreviations
BMI: body mass index; BP: blood pressure; CNS: central nervous system; CRP: C-reactive protein; CT: computed tomography; EEG: electroencephalogram; ESR: erythrocyte segmentation rate; MRA: magnetic resonance angiogram; TA: Takayasu arteritis; USS: ultrasound scan
| References | ▴Top |
- Vaideeswar P, Deshpande JR. Pathology of Takayasu arteritis: a brief review. Ann Pediatr Cardiol. 2013;6(1):52-58.
doi pubmed - Setty HSN, Vijaykumar JR, Nagesh CM, et al. Takayasu's arteritis - a comprehensive review. J Rare Dis Res Treat. 2017;2(2):63-68.
doi - Russo RAG, Katsicas MM. Takayasu Arteritis. Front Pediatr. 2018;6:265.
doi pubmed - Bond KM, Nasr D, Lehman V, Lanzino G, Cloft HJ, Brinjikji W. Intracranial and extracranial neurovascular manifestations of takayasu arteritis. AJNR Am J Neuroradiol. 2017;38(4):766-772.
doi pubmed - Kim HJ, Suh DC, Kim JK, Kim SJ, Lee JH, Choi CG, Yoo B, et al. Correlation of neurological manifestations of Takayasu's arteritis with cerebral angiographic findings. Clin Imaging. 2005;29(2):79-85.
doi pubmed - Pallangyo P, Epafra E, Nicholaus P, Lyimo F, Kazahura P, Janabi M. Bilateral ocular ischemia-induced blindness as a presenting manifestation of Takayasu arteritis: a case report. J Med Case Rep. 2017;11(1):153.
doi pubmed - Arend WP, Michel BA, Bloch DA, Hunder GG, Calabrese LH, Edworthy SM, Fauci AS, et al. The American College of Rheumatology 1990 criteria for the classification of Takayasu arteritis. Arthritis Rheum. 1990;33(8):1129-1134.
doi pubmed - Bolaman Z, Yavasoglu I, Kadikoylu G, Unubol M, Koseoglu K, Akyol A. Takayasu arteritis with intracranial involvement mimicking epilepsy: case report and review of the literature. Intern Med. 2011;50(12):1345-1348.
doi pubmed - Ioannides MA, Eftychiou C, Georgiou GM, Nicolaides E. Takayasu arteritis presenting as epileptic seizures: a case report and brief review of the literature. Rheumatol Int. 2009;29(6):703-705.
doi pubmed - Sriskantharajah S, Thambipillai P, Balasingam N. Epileptic seizure: An unusual presentation of takayasu arteritis. Int J Clin Rheumatol. 2018;13(1):60-62.
doi - Mukherjee S, Naskar A, Chatterjee A. Seizures and lost pulses: an atypical case of Takayasu's arteritis. IOSR Journal of Dental and Medical Sciences. 2014;13(10):17-19.
doi - Menon B, Himabindu A. Takayasu's disease presenting as convulsive syncope which had been misinterpreted as epilepsy: a case report. J Med Case Rep. 2010;4:352.
doi pubmed - Feddock CA. The lost art of clinical skills. Am J Med. 2007;120(4):374-378.
doi pubmed - Vukanovic-Criley JM, Criley S, Warde CM, Boker JR, Guevara-Matheus L, Churchill WH, Nelson WP, et al. Competency in cardiac examination skills in medical students, trainees, physicians, and faculty: a multicenter study. Arch Intern Med. 2006;166(6):610-616.
doi pubmed - Cook C. The lost art of the clinical examination: an overemphasis on clinical special tests. J Man Manip Ther. 2010;18(1):3-4.
doi pubmed
This article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Medical Cases is published by Elmer Press Inc.