

| Journal of Medical Cases, ISSN 1923-4155 print, 1923-4163 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Med Cases and Elmer Press Inc |
| Journal website http://www.journalmc.org |
Case Report
Volume 9, Number 10, October 2018, pages 352-354
A Case of a Subglottic Stone
Sang Hyun Nama, Kyoung Rai Chob, c
aDepartments of Plastic and Reconstructive Surgery, Sanggye Paik Hospital, Inje University School of Medicine, Seoul, Korea
bDepartments of Otolaryngology Head and Neck Surgery, Sanggye Paik Hospital, Inje University School of Medicine, Seoul, Korea
cCorresponding Author: Kyoung Rai Cho, Department of Otorhinolaryngology-Head and Neck Surgery, Sanggye Paik Hospital, Inje University School of Medicine, 761-1 Sanggye 7 Dong, NowonGu, 139 - 707, Seoul, Korea
Manuscript submitted September 21, 2018, accepted September 27, 2018
Short title: A Case of a Subglottic Stone
doi: https://doi.org/10.14740/jmc3171
| Abstract | ▴Top |
A 50-year-old woman visited our clinic, complaining of a long-term foreign body sensation in her throat. Laryngeal examination revealed a subglottic nodular lesion posterior to the anterior commissure. Her laboratory data were within normal range and there was no particular abnormality in her history. A 2-mm sized stone was extracted after incising the nodule. The surrounding nodular tissue was removed carefully. The patient recovered completely after the surgery. This is the first case of a subglottic laryngeal stone reported in an English-language journal.
Keywords: Subglottis; Stone
| Introduction | ▴Top |
The benign laryngeal mucosal lesions include vocal cord nodules, vocal cord polyps, Reinke’s edema, vocal cord cysts and granuloma [1, 2]. Hoarseness and the sensation of a foreign body in the throat are the most frequent symptoms of these disorders. A case study of a submucosal vocal cord stone has not been reported previously in English-language journals. Stones that have developed within the body are found primarily in tubular or cystic structures, such as the ureter, the gallbladder and the salivary glands [3, 4]. The prevalence of laryngeal stones is rare, because the vocal cord vibrates consistently with a fast air stream. Furthermore, there is no specific structure of the vocal cord upon which calcification can develop easily.
Herein, we report a case of a laryngeal stone found in the subglottic area of the anterior commissure.
| Case Report | ▴Top |
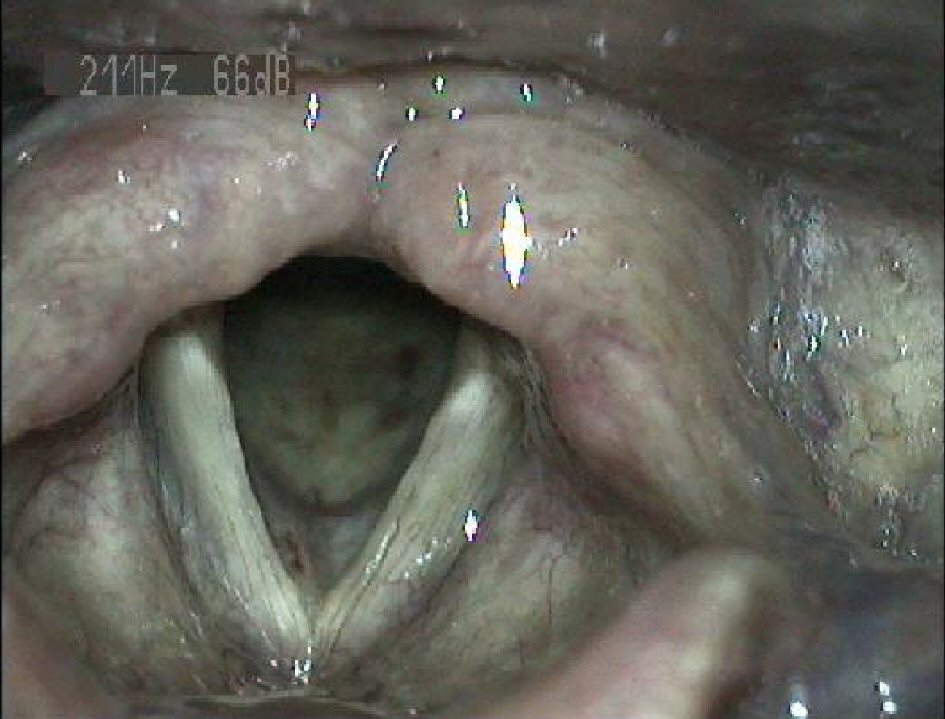
A 50-year-old woman complaining of a foreign body sensation in her throat was referred to our clinic. A laryngeal mass located in the right subglottic area was visible on laryngoscopic examination (Fig. 1). The patient had no recent operation history, except for an appendectomy under general anesthesia 30 years prior to this episode.
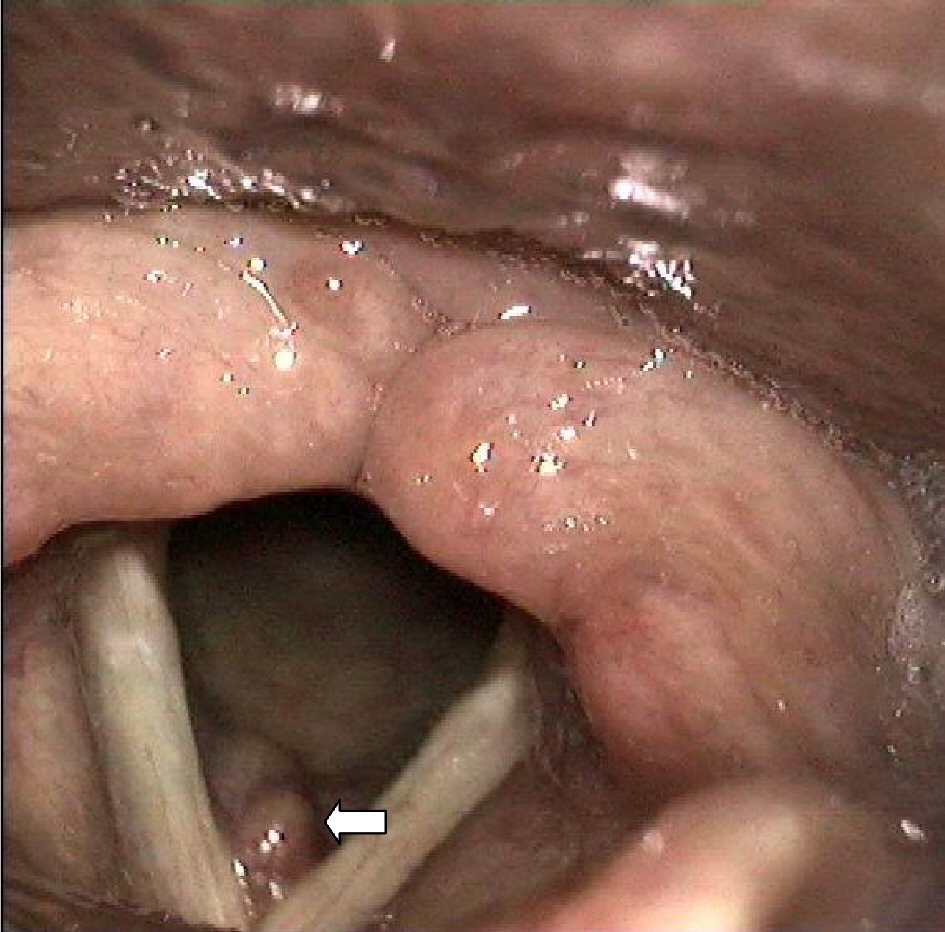 Click for large image | Figure 1. Laryngeal examination shows the mass in anterior subglottic region (arrow). |
On preoperative evaluation, the patient’s laboratory data, electrocardiogram, and chest X-ray were within normal range. She underwent a laryngeal microscopic surgery under general anesthesia. After incising the subglottic mass, a 2-mm sized yellowish stone was extracted. The surrounding soft tissue was trimmed for biopsy (Fig. 2).
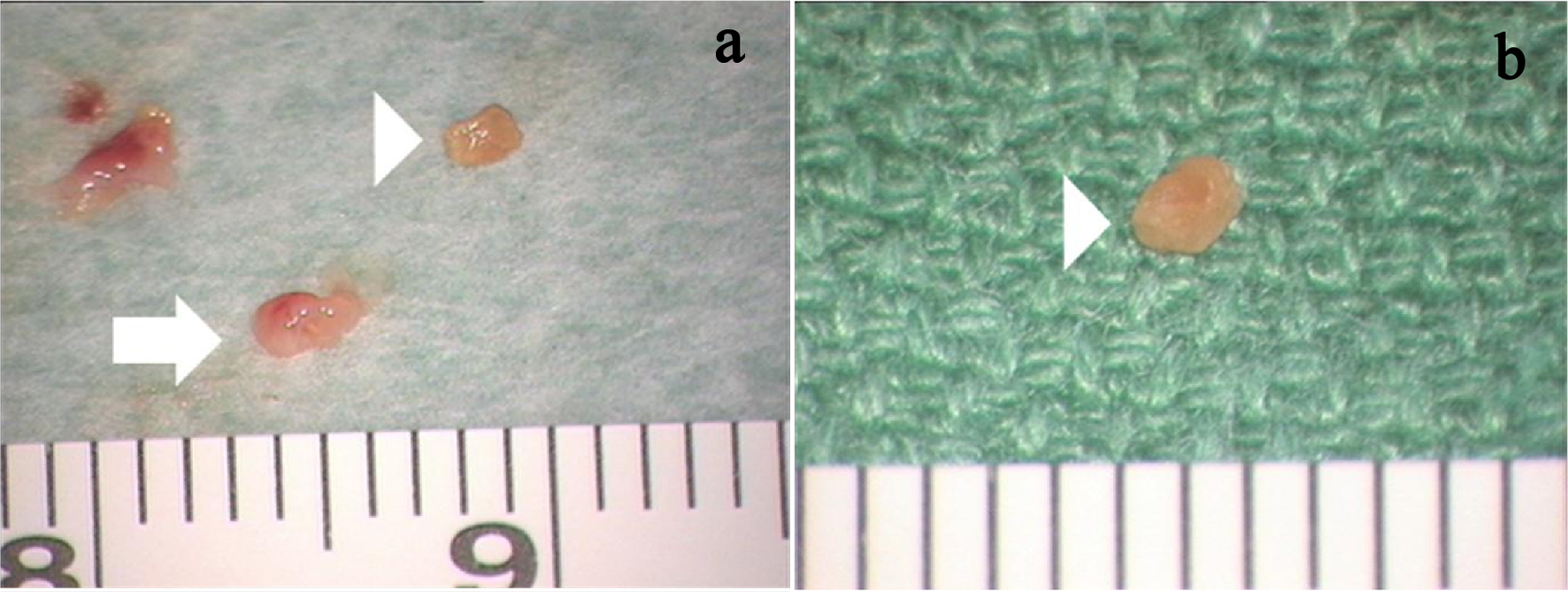 Click for large image | Figure 2. Excised mass with stone. (a) Excised mass (arrow) with stone (arrow head). (b) Extracted stone, close-up view (arrow head). |
The findings of the pathological examination reported amorphous stones of unknown components (Figs. 3, 4). To determine if this finding was the result of a metabolic disease, serum calcium level and the parathyroid hormone level were checked out; the results were within the normal ranges. The patient had completely recovered from the preoperative symptoms and her follow-up laryngeal examination was normal (Fig. 5).
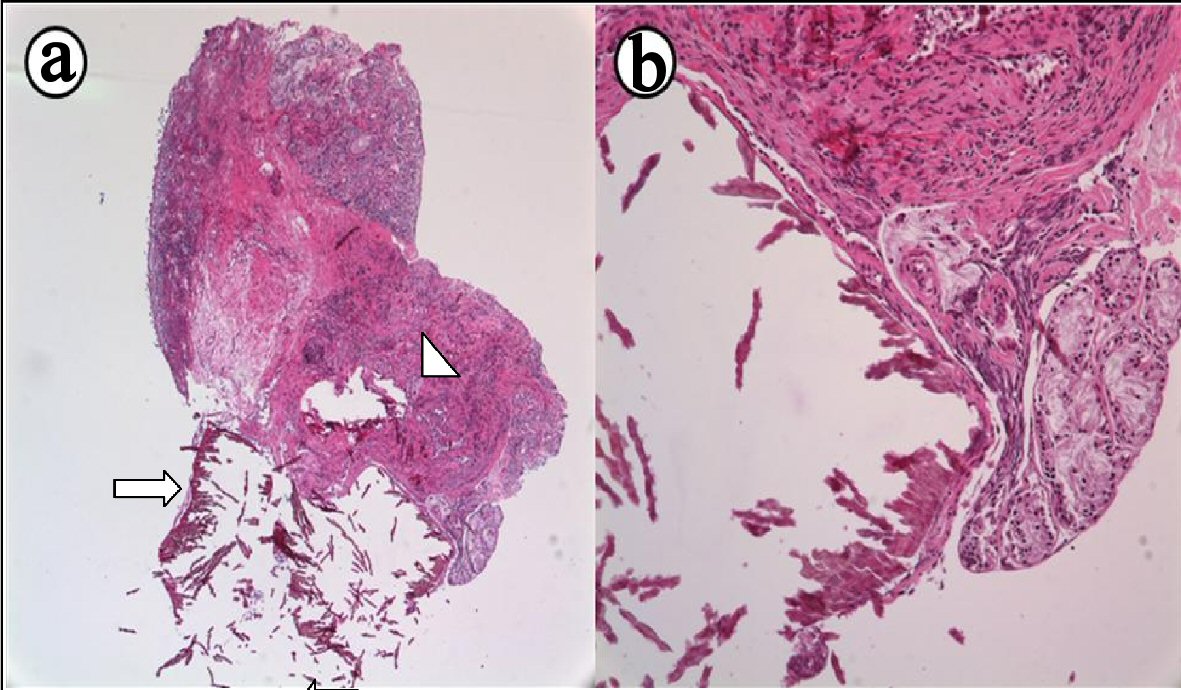 Click for large image | Figure 3. Subglottic mass with stone (arrow). Amorphous material surrounded with inflammatory tissues (arrow head). (a) H&E × 40. (b) H&E × 100. |
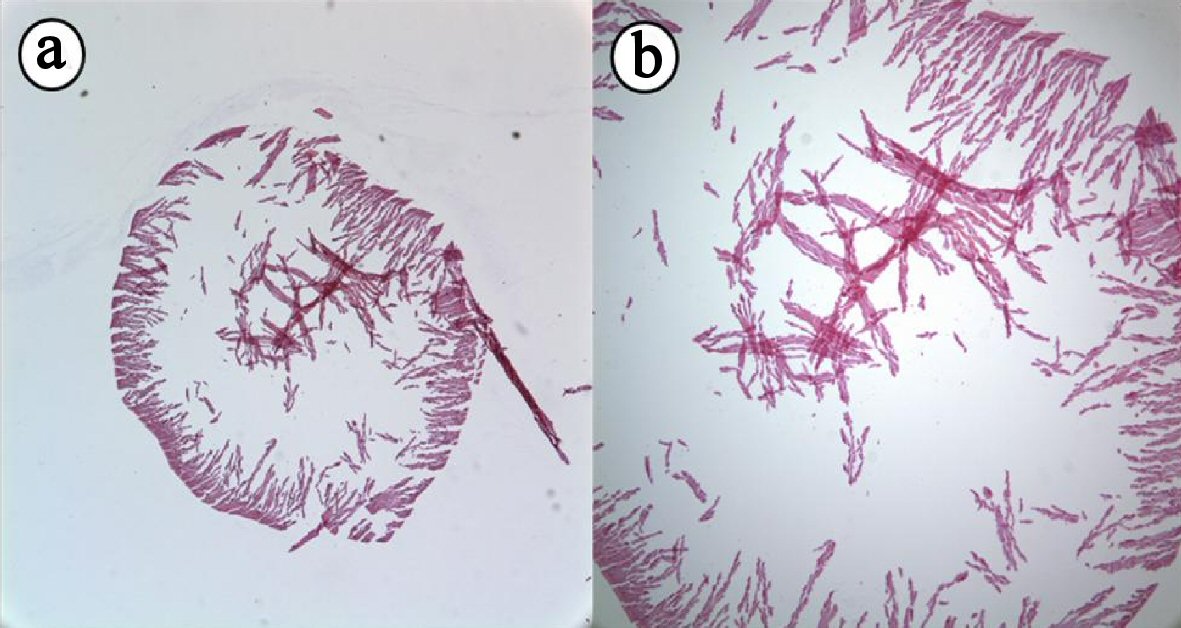 Click for large image | Figure 4. Sectioned images of extracted stone. Round amorphous stone with thick surface. Internal hallow is made by cutting artifact. (a) H&E × 40. (b) H&E × 100. |
 Click for large image | Figure 5. Laryngeal view 1 month after surgery. |
| Discussion | ▴Top |
As physicians, when we examine a protruding mass in the vocal cord, we should keep many different diseases in the diagnostic differential. The most common disorders would be highlighted in detail including vocal cord nodules and vocal polyps. Masses can develop as a result of infection, such as vocal cord cysts, granuloma, carcinoma, tuberculosis, and actinomycosis. In addition, some other masses can originate from an inflammatory reaction: lupus, sarcoidosis, or Wegener’s granuloma [1, 2]. In general, stones, which are solid concretions or crystal aggregations formed by calcification, include primarily urethra stones, gallbladder stones, salivary gland stones, and tonsiloliths [3, 4]. In the vocal cord, the prevalence of the laryngeal stones is very rare because the vocal cord consistently vibrates with a fast air stream, while a person is creating the sounds of speech. In other words, there is no specific structure in the vocal cord which contributes to form calcification and crystal aggregations because of their movement.
In patients with chronic renal failure, serum calcium and phosphate levels tend to run high over the long-term; these high levels can lead to calcification [5, 6]. In our case, the patient’s renal function, parathyroid hormone level and serum calcium level have been within normal range.
Although Hegab [7] reported laryngolith previously, it was different from this case. That stone was in the laryngeal lumen that they could see the stone itself, but our case was covered with laryngeal mucosa. According to Hegab’s study [7], the researchers reported that the laryngeal stone was the result of granulation: the granulation was generated by wounds from endotracheal intubation. In our case study, we considered the possibility that the patient’s laryngeal stone could have been formed by wounds incurred from endotracheal intubation of general anesthesia that took place during the surgery that had occurred 30 years prior. However, the soft tissue surrounding the stones was normal mucosa and it was located anteriorly in the vocal cord, away from the vocal process that is frequently injured during intubation; the specific cause for the laryngeal stone has not been identified in this case.
During medical treatment, the patient underwent mass excision under laryngeal microscopic examination, similar to other patients diagnosed with a laryngeal mass. After surgery, the patient was free from the sensation of foreign body in her throat without recurrence.
We will look forward to obtaining more research and to studying the development of laryngeal stones in depth, since sufficient studies to determine its causes and contributing factors have not been taken place.
Conflict of Interest
All authors had no conflict of interest on this study.
Declarations
All authors significantly contributed to and agreed upon the content of the manuscript.
Financial Support
There is no financial and material support or funding.
| References | ▴Top |
- Johns MM. Update on the etiology, diagnosis, and treatment of vocal fold nodules, polyps, and cysts. Curr Opin Otolaryngol Head Neck Surg. 2003;11(6):456-461.
doi pubmed - Loire R, Bouchayer M, Cornut G, Bastian RW. Pathology of benign vocal fold lesions. Ear Nose Throat J. 1988;67(5):357-358, 360-352.
- Sayer JA. Renal stone disease. Nephron Physiol. 2011;118:35-44.
doi pubmed - Williams MF. Sialolithiasis. Otolaryngol Clin North Am. 1999;32(5):819-834.
doi - Belser RB, Jr., Setrakian S, Stepnick DW, Hricik DE. Metastatic calcification of the true vocal cords as a cause of hoarseness. Ann Otol Rhinol Laryngol. 1994;103(11):849-851.
doi pubmed - Patel NP, Wright SC, Bergman S. Metastatic calcification involving the true vocal cord. Am J Otolaryngol. 2009;30(3):216-218.
doi pubmed - Hegab AH. Laryngolith. J Laryngol Otol. 2009;123(2):e9.
doi pubmed
This article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Medical Cases is published by Elmer Press Inc.