

| Journal of Medical Cases, ISSN 1923-4155 print, 1923-4163 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Med Cases and Elmer Press Inc |
| Journal website http://www.journalmc.org |
Case Report
Volume 9, Number 5, May 2018, pages 139-141
Cervical Radiculopathy Alleviating by Manipulative Correction of Cervical Hypolordosis
Eric Chun-Pu Chua, c, Taebum Lima, Kin-Cheung Makb
aNew York Chiropractic & Physiotherapy Centre, New York Medical Group, Hong Kong, China
bDepartment of Orthopaedics & Traumatology, HK University Li Ka Shing Faculty of Medicine, Hong Kong, China
cCorresponding Author: Eric Chun-Pu Chu, New York Chiropractic and Physiotherapy Centre, 41/F Langham Place Office Tower, 8 Argyle Street, Mongkok, Hong Kong, China
Manuscript submitted March 30, 2018, accepted April 9, 2018
Short title: Cervical Hypolordosis and Radiculopathy
doi: https://doi.org/10.14740/jmc3051w
| Abstract | ▴Top |
The purpose of this report is to present an interesting case of cervical radiculopathy in a patient with a prominent cervical hypolordosis treated by chiropractic adjustment. A 55-year-old office worker with severe neck pain and numbness of the right arm sought chiropractic treatment. Following 12 sessions of cervical adjustment, the patient experienced complete alleviation from radiculopathy and full restoration of cervical curvature. Neck pain is common and the cause is usually multifactorial. About 88% of uncomplicated neck pain is self-limiting. Conservative treatment is advocated as initial modality for most patients. Cervical radiculopathy, however, is a potential problem because nerve impingement can cause disability due to numbness or paresthesia, and even weakness, requiring surgical intervention. The best chance for sensorimotor recovery is with prompt intervention to decompress the pinched nerve. Instead of watchful waiting, early application of chiropractic adjustment may help release nerve impingement, and avoid medications and operations in patients with neglected nerve compression.
Keywords: Cervical hypolordosis; Chiropractic; Forward head posture; Manual adjustment; Radiculopathy
| Introduction | ▴Top |
Cervical radiculopathy refers to neurological symptoms resulting from extrinsic pressure on the root of the cervical nerve. About 78% of cases result from foraminal encroachment by degenerative bony changes [1]. Conservative approach is advocated as initial modality for most patients [2]. Surgical interventions are indicated in cases where patients remain disability and failure to respond positively to conservative care. As illustrated in reported cases [3-5], the application of chiropractic adjustments had appeared to offer an effective strategy for the alleviation of cervical radiculopathy. Correction of neck posture itself can substantially help alleviate the symptoms of cervical radiculopathy [6].
| Case Report | ▴Top |
A 55-year-old man sought chiropractic treatment after experiencing severe nuchal pain and numbness of the right arm for 6 months. He described his neck pain as a deep, dull ache accompanied by a sensation of pressure and numbness over the lateral aspect of his right upper arm. At presentation, his average pain level was rated as 7/10 on the numeric pain rating scale (NPRS). He worked a seated desk job requiring computer use of at least 9 h a day, 6 days per week. He had been taking pain relievers (ibuprofen and acetaminophen) for 6 months, but only partial relief of painful symptoms. He denied any history of trauma and had high blood pressure under controlled.
The patient presented here with several postural alterations, including forward head posture (Fig. 1a), high left shoulder and mild to moderate thoracic hyperkyphosis. Chiropractic assessment yielded joint restriction at C1/2, C5/6 and C7/T1 levels, limited cervical range of motion during extension, and pain was located at the cervicothoracic junction at spinal percussion. Decreased muscle strength at biceps and right wrist extension was observed and rated 4/5 on neurological examination. Sensory deficit was also noted along left C6 dermatome. Radiography of the cervical spine showed C4/5 disc-space narrowing, cervical spondylosis with a decreased cervical lordosis. Mild osteophyte encroachment of right C4/5 and left C5/6 neural foramina was evident on the oblique views (Fig. 2). The patient was diagnosed with cervical spondylosis with left C6 radiculopathy.
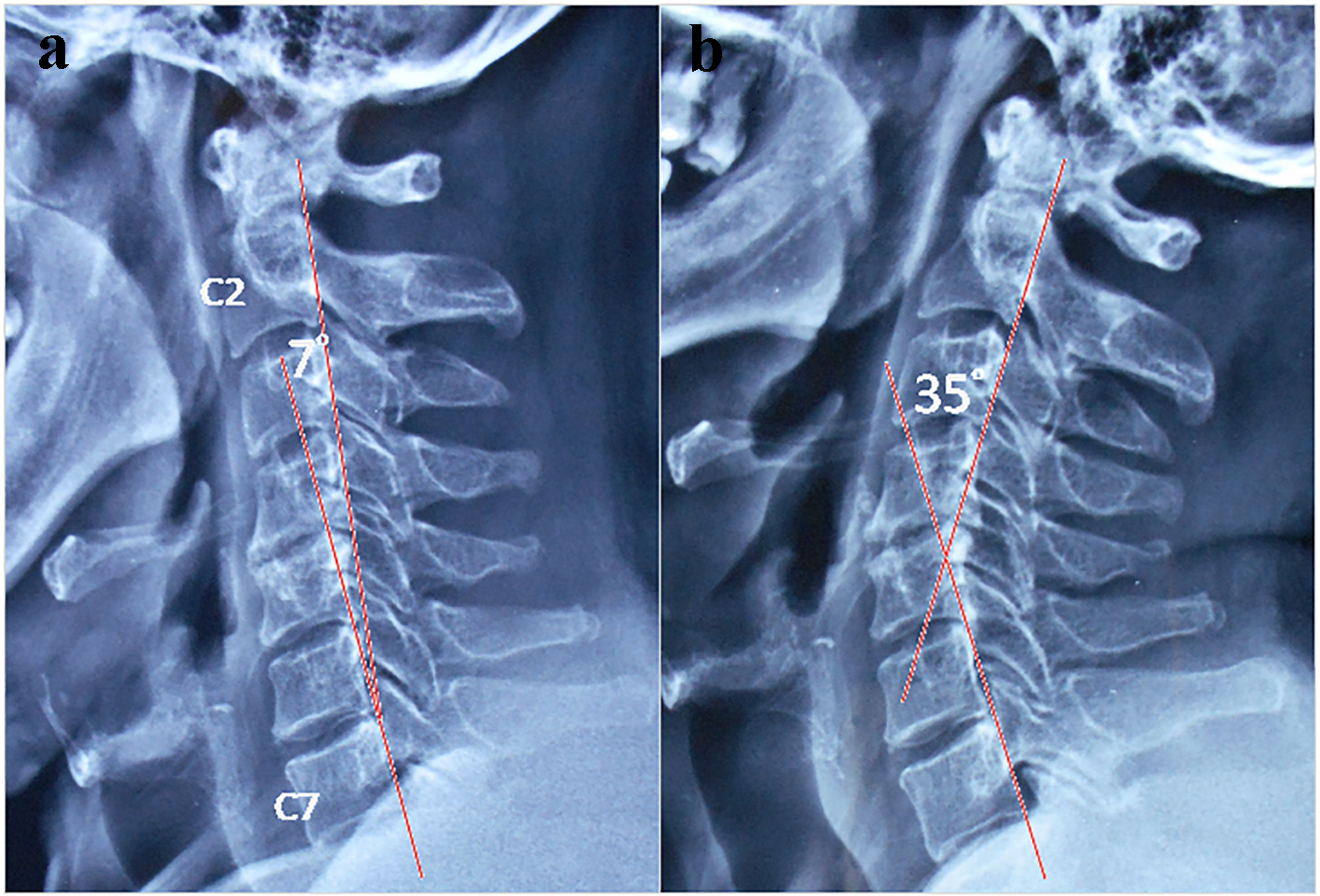 Click for large image | Figure 1. Cervical hypolordosis on lateral X-rays. (a) Pre-treatment sagittal radiograph revealed loss of cervical lordosis, with neck curvature of 7° (range: 20° to 35°). (B) Nine months later, note the restoration of cervical curvature after chiropractic treatment, measured 35° by posterior tangent method. |
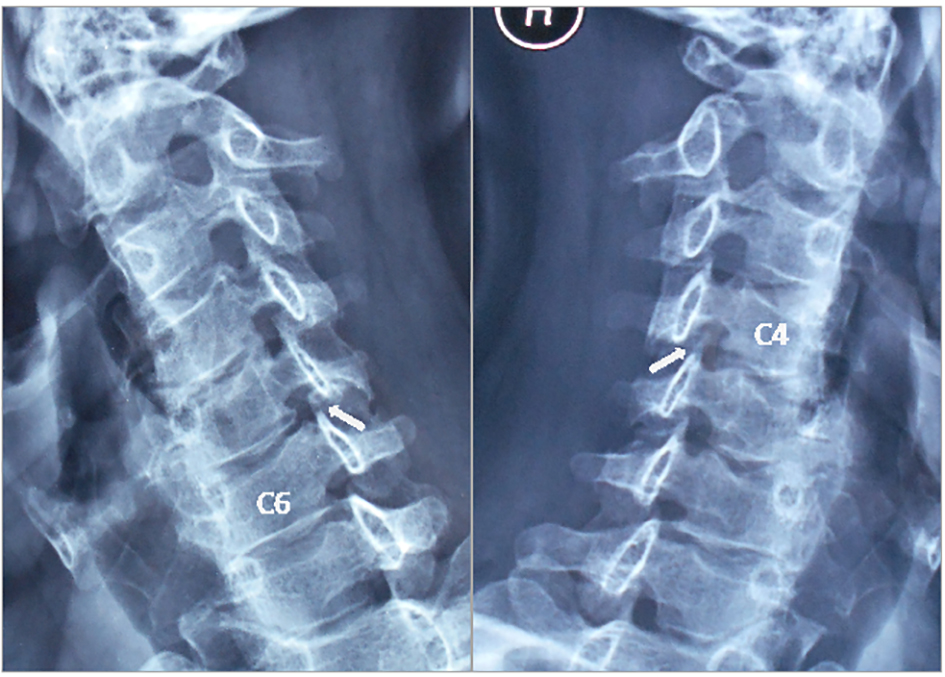 Click for large image | Figure 2. Oblique radiographs of the cervical spine. Oblique imaging demonstrating foraminal stenosis at left C5/6 and right C4/5 levels (white arrows), and evidence of cervical spondylosis, C4/5 disc-space narrowing, and a loss of cervical lordosis. |
High velocity and low amplitude manipulation adjustment, namely, diversified chiropractic technique, was used. The initial visits focused on adjusting the cervical mobility and restoring neurological function. The patient started on with thrice weekly treatments for the initial 4 weeks. His neck pain was reduced to 0/10 on NPRS and the sensorimotor deficits disappeared after the initial phase of the chiropractic care. Treatment frequency was then reduced to twice weekly for the next month, focusing on adjusting the cervical misalignment and correcting forward head posture and vertebral instability. The patient reported complete relief of pain and full mobility of his neck after completion of 2-month treatment. Restored lordotic curvature of the neck maintained and was demonstrated on X-ray at the 9-month follow-up (Fig. 1b). On 1-year follow-up over the phone, the patient remained symptom-free.
| Discussion | ▴Top |
Radiculopathy is a neurological condition where neural conduction along a spinal nerve or its roots is blocked. The majority (78%) of cervical radiculopathies result from foraminal encroachment by degenerative bony changes. Disc herniation and spinal instability consist of the remainders [1]. In acute state, radicular pain comes primarily from compression and inflammation, whereas in chronic radiculopathy, pain is usually caused by fibrosis [4]. The natural history of radiculopathy is generally thought to be favorable, and conservative approach is advocated as initial modality for most patients. Physical therapy, anti-inflammatory medications and muscle relaxants may help relieve pain. Roughly 88% of cervical radiculopathy will improve within 4 weeks of nonoperative management [7]. Surgical intervention is reserved for those with progressive neurologic deficit and failure of conservative approaches. In regard to non-operative regimen, initial care may vary significantly among practitioners. Recent studies show that a multimodal management strategy, integrating of spinal manipulation, neurodynamic mobilization and specific exercise is the more effective conservative treatment for patient with cervical radiculopathy [4, 8].
This case brings us to the question whether chiropractic manipulation can have a role in the treatment of cervical radiculopathy. Many studies have confirmed the efficacy of chiropractic adjustments in alleviating cervical radiculopathy [3-5]. Of the review of 162 consecutive patients diagnosed with upper or lower extremity radiculopathy, 85.5% had resolution of radicular complaints after chiropractic treatment [4]. Ninety-one percent of acute presentations (symptom duration < 3 months, n = 67) resolved with a mean treatment trial of 6.2 sessions, and 81% of chronic presentations (symptom duration > 3 months, n = 95) resolved with a mean treatment trial of 8.6 sessions [4]. Putative mechanisms behind chiropractic effects on pain relief include reduced muscle hypertonicity via stretching, disruption of periarticular restrictions [9], and release of the entrapped tissues [10]. A recent MRI study has demonstrated increased gapping of the zygapophyseal joints after spinal adjustment [11], which further supports the hypothesis that chiropractic adjustments break up adhesions and promote circulation in tight and inflamed joints, connective tissues, and the histologic components of vertebral subluxation complex, respectively [12].
It is also interesting to note with regard to restoration of neck curvature in alleviating cervical radiculopathy. Cervical hypolordosis describes a deficient front-to-back spinal curvature in the neck. In general, normal values have been reported to range from 20° to 35° for C2 to C7 [13]. A study conducted in 369 subjects of different occupations, researchers observed that cervical hypolordosis is the commonest defect, which leads to painful neck syndrome and to serious compression of cervical nerve roots [14]. Previous studies showed length changing of the spinal cord in flexion and extension. The average length is around 1.5 cm yielded in the cervical segment [15]. It is apparent to realize that there are tension points in the body, such as the intervertebral foramen, where the nerve/interface relationship is constant during movement and may be vulnerable to nerve compression [16]. Thence, it is reasonable to believe that correcting the hypolordotic curvature (forward head posture) by cervical adjustment may help reduce the spinal nerve tension, release its pinched nerve, and subsequently alleviate arm numbness and muscle weakness in this patient. Similar therapeutic outcome for cervical radiculopathy had been reported recently by correcting a lateral head posture [6].
Nerve impingement is a potential problem in patients with radiculopathy, since it can cause disability requiring nerve root decompression. As illustrated in this report, the application of chiropractic adjustments appeared to offer a treatment efficacy for radicular pain and cervical hypolordosis. Chiropractic adjustment would appear to be one of the leading nonoperative regimens for preventing morbidities and avoiding unnecessary medication and surgery in patients with cervical radiculopathy. The main limitation of this report is that therapeutic mechanisms responsible for manipulative effects remain unclear. Furthermore, there are no comparison groups to supply evidence that chiropractic is superior to other regimens. This single case report is not proof of concept, but patients’ experiences are supportive [3-6]. Further studies regarding the efficacy of other conservative approach for radiculopathy are needed to guide treatment selection.
Conclusion
Cervical radiculopathy can be a serious problem, since neural impingement can cause sensory or motor disability. Early application of chiropractic adjustments that help with releasing nerve impingement and restoring sensorimotor function and head posture could be considered.
Conflict of Interest
The authors declare no conflict of interest.
| References | ▴Top |
- Kim KT, Kim YB. Cervical Radiculopathy due to Cervical Degenerative Diseases : Anatomy, Diagnosis and Treatment. J Korean Neurosurg Soc. 2010;48(6):473-479.
doi pubmed - Spurling RG, Segerberg LH. Lateral intervertebral disk lesions in the lower cervical region. J Am Med Assoc. 1953;151(5):354-359.
pubmed - Murphy DR, Hurwitz EL, Gregory A, Clary R. A nonsurgical approach to the management of patients with cervical radiculopathy: a prospective observational cohort study. J Manipulative Physiol Ther. 2006;29(4):279-287.
doi pubmed - Christensen KD, Buswell K. Chiropractic outcomes managing radiculopathy in a hospital setting: a retrospective review of 162 patients. J Chiropr Med. 2008;7(3):115-125.
doi pubmed - Peterson CK, Schmid C, Leemann S, Anklin B, Humphreys BK. Outcomes from magnetic resonance imaging-confirmed symptomatic cervical disk herniation patients treated with high-velocity, low-amplitude spinal manipulative therapy: a prospective cohort study with 3-month follow-up. J Manipulative Physiol Ther. 2013;36(8):461-467.
doi pubmed - Berry RH, Oakley P, Harrison D. Alleviation of radiculopathy by structural rehabilitation of the cervical spine by correcting a lateral head translation posture (-TXH) using Berry translation traction as a part of CBP methods: A case report. Chiropr J Australia. 2017;45(1):63-72.
- Thoomes EJ. Effectiveness of manual therapy for cervical radiculopathy, a review. Chiropr Man Therap. 2016;24:45.
doi pubmed - Chu ECP. Chiropractic care of postlaminectomy syndrome: A report of 2 cases. Int J Med Health Sci. 2017;6(3):185-187.
- Chu ECP, Wong RSM. Chiropractic pain control in myelofibrosis: A case report. New Horizons Clin Case Reports. 2017;2:7-9.
doi - Crame GD, Tuck NR, Knudsen JT, Fonda SD, Schliesser JS, Fournier JT, et al, Effects of side-posture positioning and side-posture adjusting on the lumbar zygapophyseal joints as evaluated by magnetic resonance imaging: a before and after study with randomization. J Manipulative Physiol Ther. 2000;23:380-394.
doi pubmed - Cailliet R, Gross L. The Rejuvenation Strategy. 1st edn. New York: Doubleday & Co.; 1987. p. 50-59.
- Gore DR, Sepic SB, Gardner GM. Roentgenographic findings of the cervical spine in asymptomatic people. Spine (Phila Pa 1976). 1986;11(6):521-524.
doi - Choudhary BS, Sapur S, Deb PS. Forward head posture is the cause of 'straight spine syndrome' in many professionals. Indian J Occup Environ Med. 2000;4(3):122-124.
- Frostell A, Hakim R, Thelin EP, Mattsson P, Svensson M. A review of the segmental diameter of the healthy human spinal cord. Front Neurol. 2016;7:238.
doi pubmed - Butler DS. Adverse mechanical tension in the nervous system: a model for assessment and treatment. Aust J Physiother. 1989;35(4):227-238.
doi
This article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Medical Cases is published by Elmer Press Inc.