

| Journal of Medical Cases, ISSN 1923-4155 print, 1923-4163 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Med Cases and Elmer Press Inc |
| Journal website http://www.journalmc.org |
Case Report
Volume 5, Number 9, September 2014, pages 491-494
Experience With Surgery for Synchronous Metastatic Lung Tumors From Colon and Thyroid Cancer
Yasumichi Yamamotoa, b, Toshiya Tosazakia, Shinji Kosakaa
aDepartment of Thoracic Surgery, Shimane Prefectural Central Hospital, Shimane, Japan
bCorresponding Author: Yasumichi Yamamoto, Department of Thoracic Surgery, Shimane Prefectural Central Hospital, 4-1-1 Himebara, Izumo, Shimane 693-8555, Japan
Manuscript accepted for publication August 7, 2014
Short title: Double Lung Metastases
doi: https://doi.org/10.14740/jmc1913w
| Abstract | ▴Top |
Chest computed tomography (CT) demonstrated a solitary nodular shadow in the right middle lobe of the lung of a 74-year-old woman. She had undergone hemithyroidectomy for sclerosing follicular thyroid carcinoma 26 years ago and right hemicolectomy and sigmoidectomy for multicentric colon cancer 2 years ago. The clinical diagnosis of the lung nodule was a metastatic lung tumor from the former colon cancer. Wide wedge resection of right S4a was performed. Pathological diagnosis revealed not only the metastatic colon cancer with the interlobular lymph node involvement but also an incidental metastatic thyroid papillary carcinoma. Completion total thyroidectomy and regional lymph node dissection were performed subsequently, and this revealed primary multiple occult papillary carcinomas in the residual thyroid. This was a very rare case in which an incidental metastatic lung lesion of thyroid cancer was revealed in a specimen of resected lung metastasis from colon cancer, and led to treatment of the second primary thyroid cancer.
Keywords: Metastatic lung tumor; Double cancer; Thyroid cancer; Colon cancer; Incidental metastases
| Introduction | ▴Top |
Cancer patients tend to have a high risk of occurrence of secondary cancers in other organs. Our daily experiences of management of double cancer have been increasing as a result of innovations in diagnostic methods and treatment. The lung is one of the most frequent sites for metastatic spread of cancer of the various organs because of its rich capillary bed and central location in the circulatory system [1]. We report a rare surgical experience of synchronous lung metastasis from colon cancer and occult thyroid cancer.
| Case Report | ▴Top |
A 74-year-old woman showing surgical scars from previous procedures, but without any subjective symptoms, presented for a normal physical examination. She had undergone right hemi-thyroidectomy for sclerosing follicular thyroid carcinoma in 1986, and right hemicolectomy and sigmoidectomy for multicentric pT3N1-aM0 stage IIIb and pT2N1M0 stage IIIa colon cancer, respectively, in February 2010 (Fig. 1a, b). She had received UFT and Krestin as adjuvant therapy for thyroid cancer until 1987, and adjuvant chemotherapy with folic acid, fluorouracil and oxaliplatin for the colon cancer until August 2010. An 11 mm granule evident in the right lung on computed tomography (CT) was diagnosed as a metastasis from the colon cancer (Fig. 2a-c). Wedge resection of the lung with interlobular lymphadenectomy was therefore performed in July 2012.
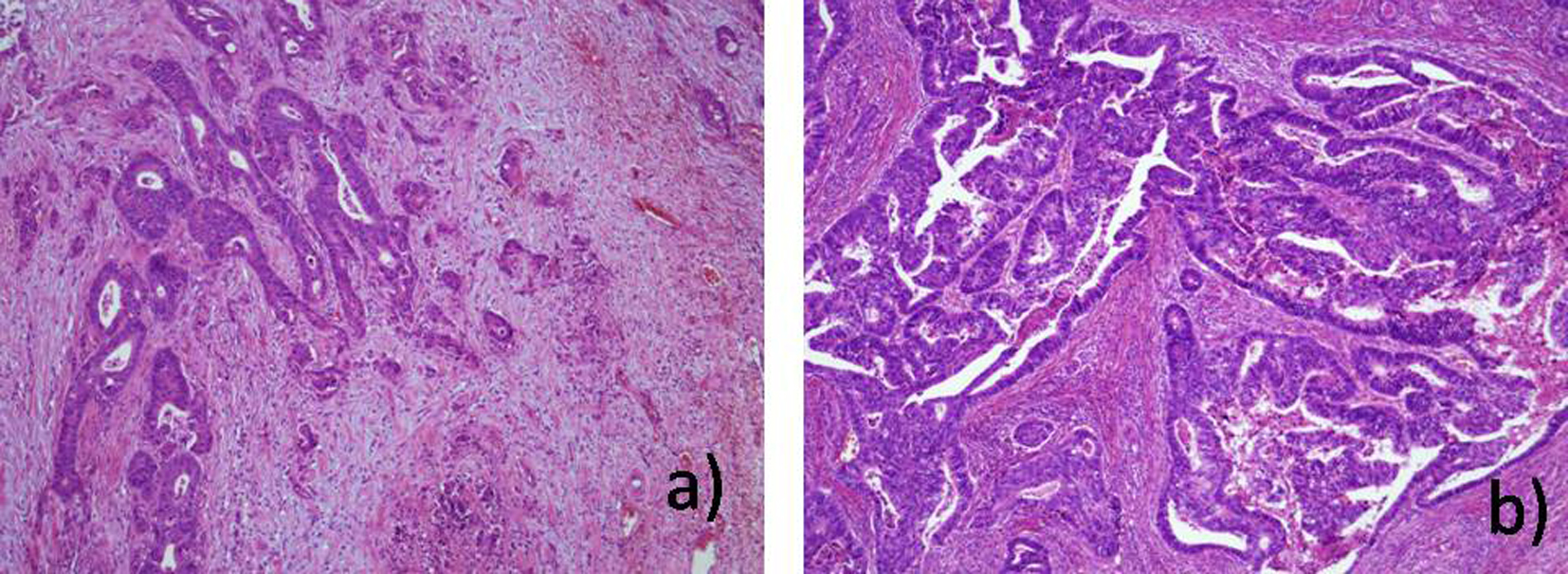 Click for large image | Figure 1. Pathological findings of colon (a) and sigmoid (b) cancer in February 2010. |
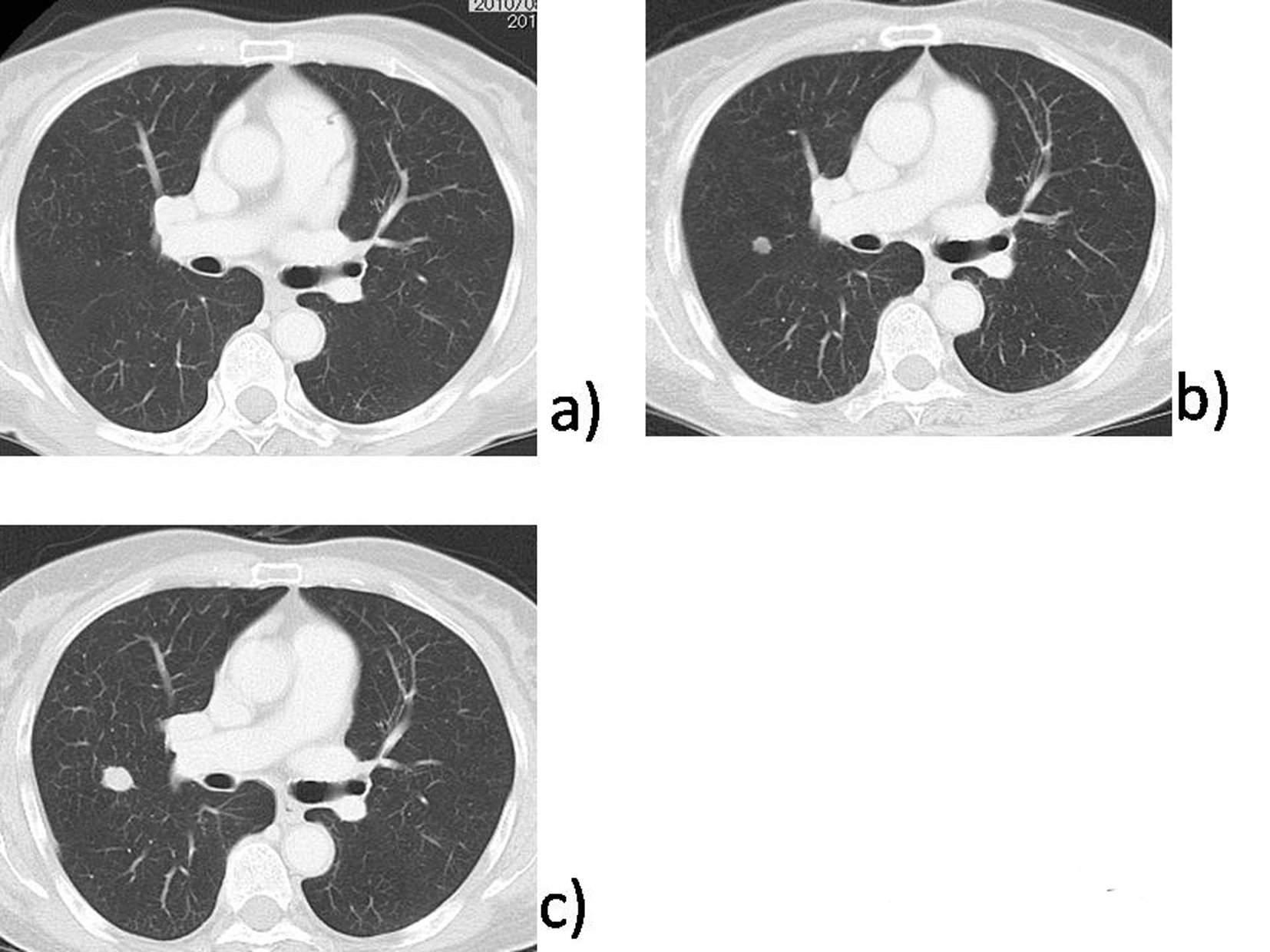 Click for large image | Figure 2. (a) A small granular shadow at S4 in the right lung in August 2010. (b) The granular shadow had grown to a nodular shadow 7 mm in diameter by August 2011. (c) Finally, the nodular shadow had enlarged to 11 mm in diameter by May 2012. |
Pathological examination revealed not only the colon cancer metastasis with lymph node involvement but also an unexpected metastatic thyroid papillary carcinoma (Fig. 3a-d).
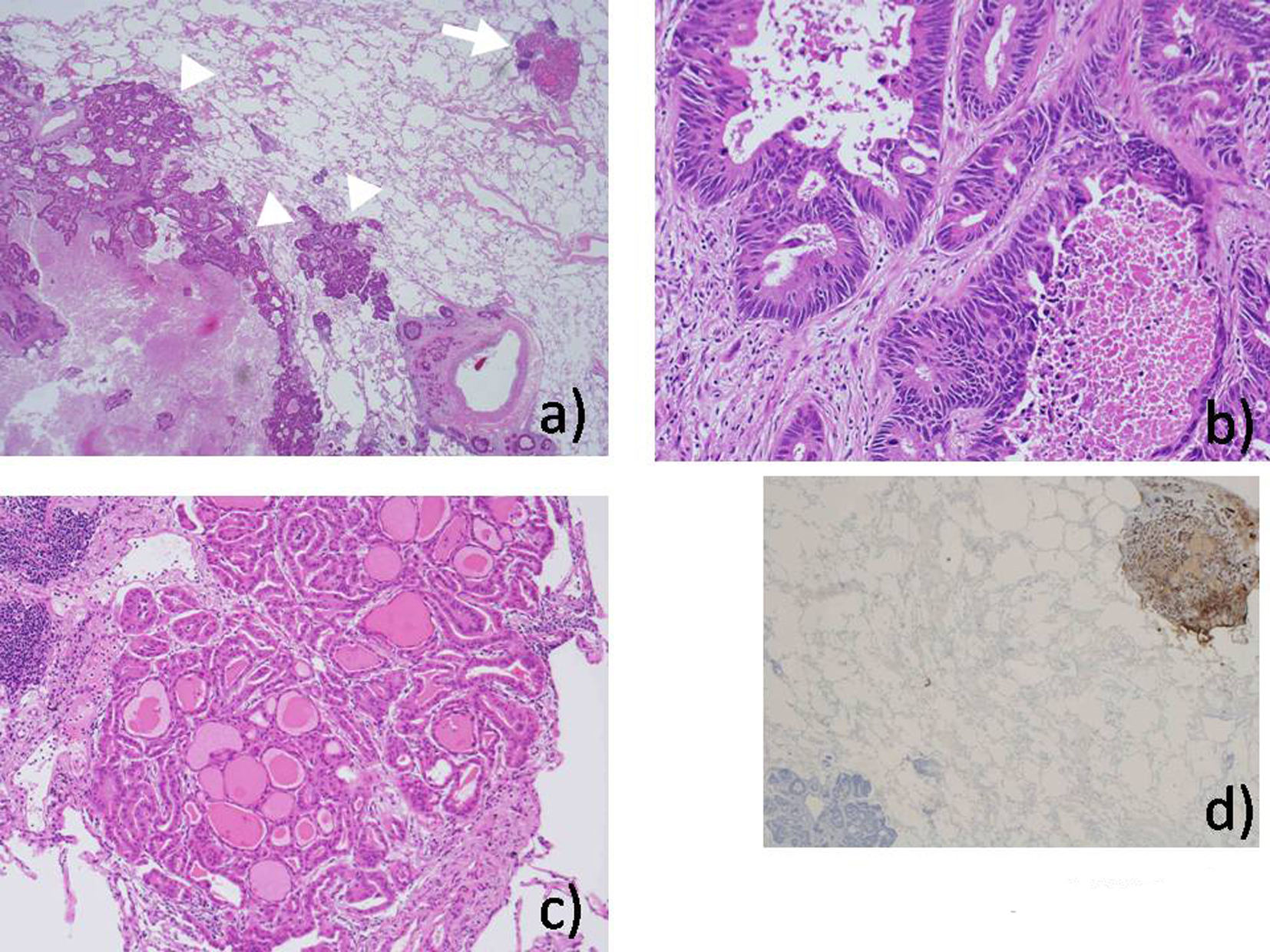 Click for large image | Figure 3. (a) A metastatic intestinal adenocarcinoma (arrow heads) and an unexpected 2 × 2 mm small nest of metastatic thyroid carcinoma (arrow) were revealed in the resected lung. (b) Tub-2 adenocarcinoma was similar to the primary lesion in the colon. The papillary carcinoma was similar to the second primary thyroid carcinoma (c), and positive for thyroglobulin (d). |
Completion thyroidectomy with regional lymph node dissection was performed in September 2012 and this revealed multiple primary pT1bN0M1 stage IVc papillary carcinomas (Fig. 4a, b).
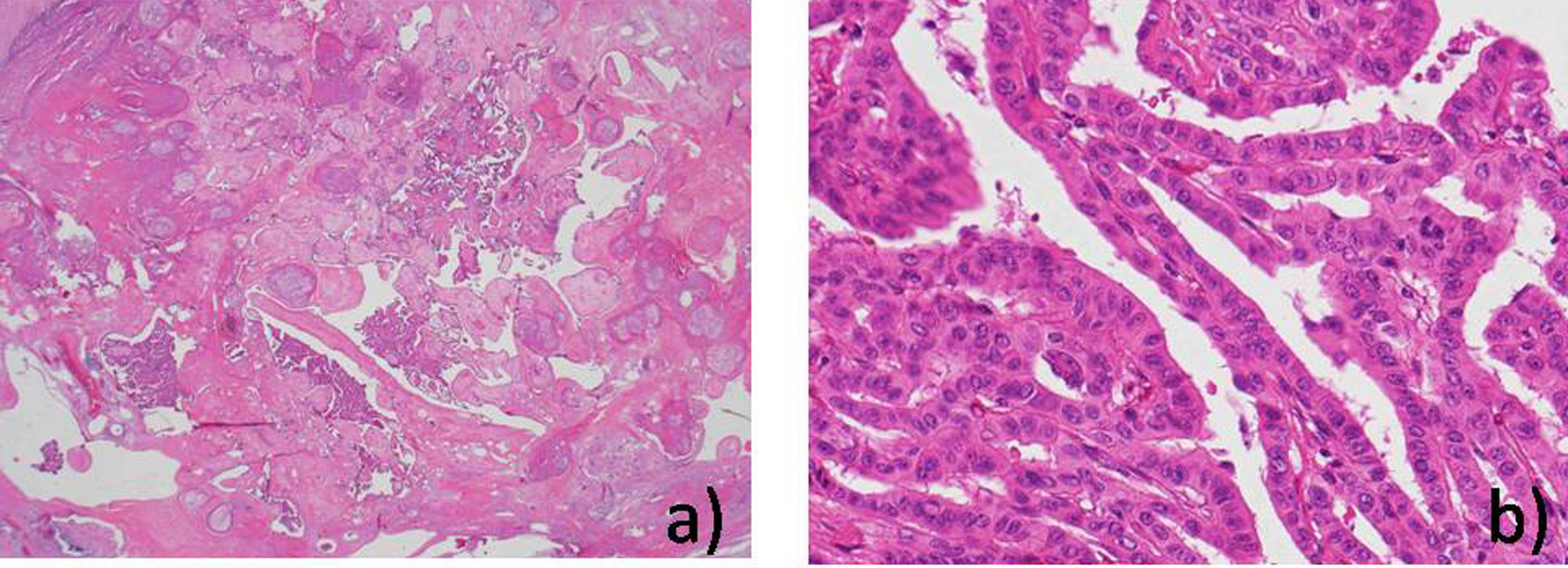 Click for large image | Figure 4. (a, b) Pathological findings of the second primary thyroid cancer in September 2012. |
In November 2013, a newly developed nodule in the right lung evident on CT was diagnosed as recurrent colon cancer in clinical setting. Chemotherapy with irinotecan, S-1 and bevacizumab was administered from January to June 2014, and five cycles were completed without disease progression.
| Discussion | ▴Top |
In view of the pathological differences, it appeared that the incidental metastasis of the lung had originated from the newly developed papillary thyroid carcinomas, and not from the previous sclerosing follicular carcinoma. Coincidental occurrence of lung or mediastinal lymph node metastasis from occult thyroid cancer and “primary” lung cancer, and also collision tumor of the metastatic lung tumor from an adenoid cystic carcinoma and the “primary” lung cancer has been reported previously [2-4]. Another report has documented metachronous resection of lung metastases from cancers of the colon and kidney [5]. The present case was a rare one in which a synchronous lung metastasis from thyroid cancer was revealed in the same specimen as a metastasis from colon cancer, and this led to surgical treatment of the second primary thyroid cancer.
Conflict of Interest
Yasumichi Yamamoto and the other co-authors have no conflicts of interest to declare.
Funding Support
None.
| References | ▴Top |
- Suster S, Moran CA. Unusual manifestations of metastatic tumors to the lungs. Semin Diagn Pathol. 1995;12(2):193-206.
pubmed - Xue L, Luan Z, Liu Y, Zou S, Jiang J, Wu N, Lu N,
et al . Pulmonary metastasis of a papillary thyroid carcinoma and primary lung adenocarcinoma: two coincident carcinomas at the same location. Diagn Pathol. 2013;8:26.
doi pubmed - Higashiyama M, Kodama K, Yokouchi H, Takami K, Motomura K, Inaji H, Koyama H. Mediastinal lymph node involvement as the initial manifestation of occult thyroid cancer in the surgical treatment of lung cancer: report of a case. Surg Today. 1999;29(7):670-674.
doi pubmed - Blanco M, Garcia-Fontan E, Rios J, Rivo JE, Fernandez-Martin R, Canizares MA. Pulmonar collision tumor: metastatic adenoid cystic carcinoma and lung adenocarcinoma. Rev Port Pneumol. 2012;18(1):42-45.
doi pubmed - Vaghei R, Harrison I, Morales N. Surgical management of multiple lung metastases of different origin. Surgery. 1989;105(6):797-800.
pubmed
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Medical Cases is published by Elmer Press Inc.