

| Journal of Medical Cases, ISSN 1923-4155 print, 1923-4163 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Med Cases and Elmer Press Inc |
| Journal website http://www.journalmc.org |
Case Report
Volume 5, Number 3, March 2014, pages 171-173
An Unusual Cause of Neck Pain: Acute Calcific Tendinitis of the Longus Colli
Elise Rodriguea, b, Jean-Pascal Costaa
aInternal Medicine Departement, Notre-Dame Hospital, Centre Hospitalier de l’Universite de Montreal, Canada
bCorresponding author: Elise Rodrigue, Internal Medicine Departement, Notre-Dame Hospital, Centre Hospitalier de l’Universite de Montreal, Canada
Manuscript accepted for publication January 14, 2014
Short title: Acute Calcific Tendinitis of the Longus Colli
doi: https://doi.org/10.14740/jmc1600w
| Abstract | ▴Top |
Calcific tendinitis of the longus colli muscle is a rare, but probably underrecognized form of calcium hydroxyapatite deposition disease. Patients present with severe neck pain, neck stiffness, odynophagia and mildly elevated inflammatory markers. This self-limited condition can easily mimic other serious diseases, such as retropharyngeal abscess, meningitis, infectious spondylodiscitis or cervical fracture. It is therefore important to promptly recognize this benign disease to avoid unnecessary and invasive tests and procedures. We present the case of a 34-year-old woman who developed acute calcific tendinitis of the longus colli following a tick bite to the neck.
Keywords: Calcific tendinitis; Neck pain; Longus colli tendinitis; Tick bite
| Introduction | ▴Top |
Few cases of calcific tendinitis of the longus colli have been described in the literature of specific specialities, notably radiology and otorhinolaryngology. However, this entity is not well known by general practitioners and internists who may encounter this rare, but underrecognized, disease. Given its tendency to mimic severe, and sometimes life-threatening conditions, we believe that physicians of all specialities should be aware of this entity in order to avoid unnecessary and invasive procedures.
| Case Report | ▴Top |
The patient, a 34-year-old woman, presented to our hospital for severe neck pain, restricted neck movements and odynophagia. She was an office worker, previously known only for accompanied migraines and remote appendicectomy and tonsillectomy. She did not take any regular medication and her life habits were unremarkable. She presented to the hospital with a 4-day history of severe neck pain radiating to her left arm, without paresia. The pain was accompanied by important limitation in neck movements in all directions. She reported a concomitant headache without sono or photophobia and of different quality than her usual migraines. She had tried anti-inflammatories, muscle relaxants, physiotherapy and acupuncture without success. In the last 2 days, she had noticed a new onset dysphagia and odynophagia with a choking sensation when she was lying on her back. She denied any fever, chills or recent infection. There was no history of trauma. However, she mentioned that, 2 weeks prior, while hiking in the woods, she had suffered a tick bite to the anterior neck. She had removed the tick herself, less than 3 h after its installation. The next day she had felt pruritis and irritation at the site of the tick bite, which quickly resolved. No rash or erythema migrans was noticed in the weeks following the incident. Upon examination, the patient was not toxic and appeared well. She was afebrile and eupneic. No stridor was heard. She noticeably held her neck very still and was not able to rotate it more than 5° in any direction. She could do a neck flexion of about 70°, but could not extend her neck. Paraspinal neck palpation was painful. There was no sensitive or motor deficits in the arms, and the reflexes were normal. The throat was exempt of erythema and swelling. No rash was noted. The rest of the examination was normal.
Her labs revealed a slight neutrophilic leucocytosis at 12.8 (N: 4-11). Hemoglobin and platelets were within the normal range. There was a mild elevation in the sedimentation rate at 24 (N: 0-20) and in the CRP at 23.8 (N: < 5). Neck X-rays were performed and revealed a thickening of the prevertebral soft tissues up to 8.2 mm at the level of C1 (Fig. 1). A CT-scan of the neck showed a fluid infiltration in the retropharyngeal space, without abscess formation. There were calcifications at the insertion site of the longus colli muscle in front of C1 (Fig. 2). Based on the clinical presentation and the pathognomonic findings on the CT-scan, a diagnosis of acute calcific tendinitis of the longus colli was made. The patient was treated with one dose of dexamethasone and diphenhydramine followed by a 2-week course of anti-inflammatories. She was released from the hospital on her second day, having improved with the dexamethasone. The patient brought the tick she had removed for analysis and it was confirmed to be an ixodes scapularis. The PCR of the tick was negative for borrelia burgdorferi and anaplasma phagocytophilum.
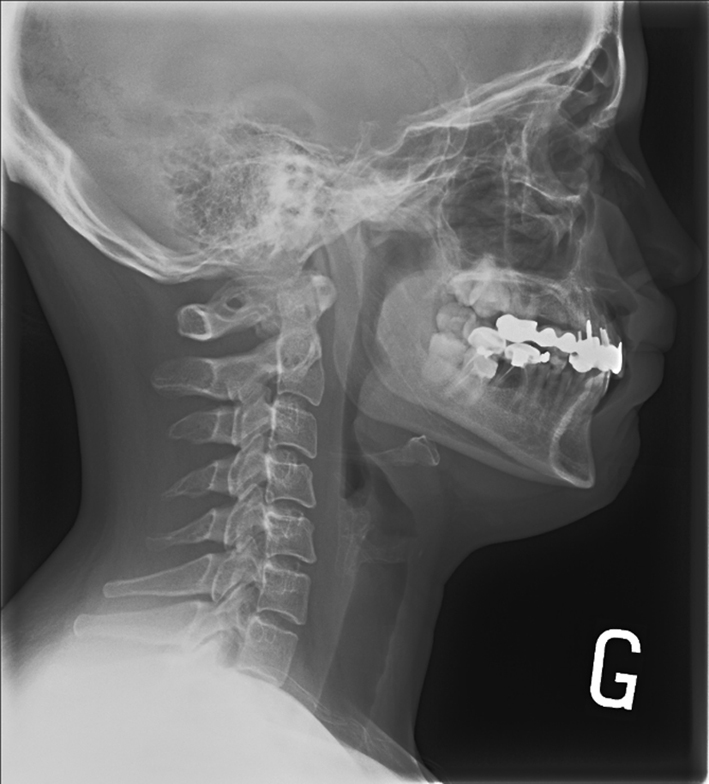 Click for large image | Figure 1. Soft tissue X-ray of the neck showing thickening of the prevertebral soft tissue, up to 8.2 mm at the level of the atlas. |
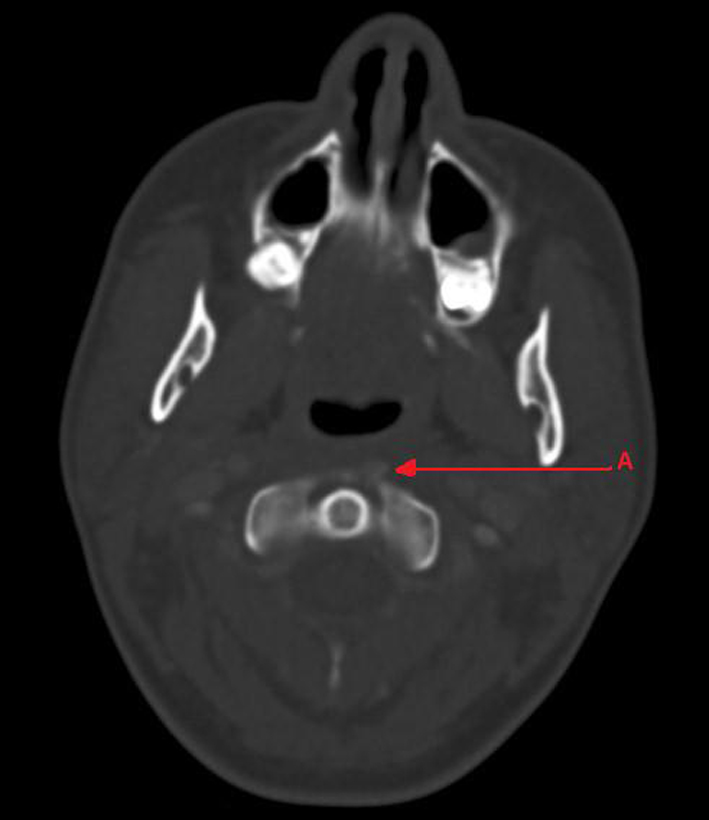 Click for large image | Figure 2. CT-scan of the neck showing calcifications (A) at the site of insertion of the longus colli tendon anterior to C1. A slight edema in the retropharyngeal space, without peripheral enhancement, is also noted. |
| Discussion | ▴Top |
Neck pain is a relatively common patient complaint. Some accompanying features such as fever and dysphagia suggest a more severe and worrisome cause of neck pain. Given its propensity to present that way, calcific tendinitis of the longus colli should be recognized when characteristic features are present. This condition is a rare, but probably underrecognized [1] form of calcium hydroxyapatite deposition disease [2]. The entity was first described by Hartley in 1964 [3] and later proven histologically to be due to calcium hydroxyapatite by Ring and his colleagues in 1994 [4]. The incidence of calcific tendinitis of the longus colli muscle is unknown. It is estimated by some to be around 0.5 per 100,000 persons per year [1], but is probably underestimated because it is a little known self-limiting entity. As in the other forms of calcium hydroxyapatite deposition disease [2], its cause is incompletely understood. It has been speculated that crystal deposition may occur following injury, tissue necrosis, ischemia and repetitive trauma. The longus colli muscle is a weak neck flexor that is one of the four anterior vertebral muscles. It extends from the anterior tubercle of C1 to the vertebral body of T3 and comprises three components: the superior, central and inferior fibers [5]. The superior fibers are the most commonly affected by the calcium hydroxyapatite deposits. The proposed mechanism is one similar to its correlates in other locations, that is, rupture of the calcific crystals leads to inflammation in the tendon. In longus colli tendinitis, a reactive effusion occurs in the retropharyngeal space, which is separated from the prevertebral space by the deep cervical fascia [2-6].
This condition affects men and women from age 21 to 81, but typically presents between the third and sixth decades [7]. The case described here presented with the characteristic triad of severe neck pain, neck stiffness and dysphagia and/or odynophagia [8]. However, our patient did not have the low-grade fever found in other cases. Upon examination, patients have very limited neck range of motion in all directions. The head is held in slight flexion. There may be posterior pharyngeal erythema or edema [6]. Blood work may show slightly elevated sedimentation rate and CRP and mild leucocytosis [9]. A history of minor trauma or upper respiratory tract infection in the prior weeks is often, but not always, present. In this case, the patient presented with a history of a recent tick bite to the neck. No case of acute calcific tendinitis of the longus colli following a tick bite was reported in the literature. However, we think that it is possible that the neck tick bite was the initiator of the inflammatory reaction in our patient. The short duration of tick attachment and the analysis of the tick support the absence of a tick-borne disease to explain the patient symptoms.
The clinical presentation of calcific tendinitis of the longus colli may suggest other worrisome diagnosis such as retropharyngeal abscess, meningitis, infectious spondylodiscitis or cervical fracture if there is a history of trauma [10]. Similarly, our patient’s symptoms evoked the possibility of a retropharyngeal abscess. Prompt recognition of this benign condition is important to avoid unnecessary and invasive tests and procedures. The diagnosis can be suspected by the presence of calcifications anterior to C1-C2 on plain neck radiographs. In our case, it was this astute observation by the radiologist that led us to the diagnosis (Fig. 1). However, the sensitivity of neck X-rays is low and the gold standard for the diagnosis is a CT-scan of the neck. The characteristic findings on CT are as follows: 1) pathognomonic calcifications in the superior fibers of the longus colli muscle; 2) fluid effusion without ring enhancement in the retropharyngeal space; and 3) exclusion of an infectious process or fractures by the absence of retropharyngeal lymph nodes and the absence of destructive changes in the adjacent anterior vertebral body [5]. The pathognomonic calcifications on the neck CT-scan of our patient in fact confirmed the diagnosis (Fig. 2). MRI of the neck may be useful in distinguishing reactive effusion from abscess in the retropharyngeal space, but is much less accurate in identifying the calcifications, and for this reason, the CT scan remains the first choice of imaging modality [11]. Calcific tendinitis of the longus colli is a benign auto-resolutive disease over the course of 2-3 weeks. However, patients are often severely limited by the neck pain and dysphagia; therefore, a short course of conservative treatment with anti-inflammatory drugs and mechanical avoidance of movement with or without a soft collar is recommended. Corticosteroids may be used for severe cases [7]. Since our patient had failed low-dose anti-inflammatories and presented with bothersome dysphagia, neck pain and chocking sensation, we chose to administer one dose of dexamethasone, which rapidly improved her symptoms. No follow-up is usually necessary for calcific tendinitis of the longus colli. If the symptoms persist for longer than 2-3 weeks, an alternative diagnosis should be sought.
In conclusion, acute calcific tendinitis of the longus colli is an underrecognized cause of severe neck pain and odynophagia that may be confounded with more severe conditions. Its pathognomonic appearance on neck CT-scan should be sought in order to avoid unnecessary or invasive procedures and to promptly begin a symptomatic treatment.
Acknowledgments
We would like to acknowledge the contribution of the Radiology Department at Notre-Dame Hospital for the interpretation of this patient’s imagery.
Conflict of Interest
No grant or conflict of interest to declare.
| References | ▴Top |
- Horowitz G, Ben-Ari O, Brenner A, Fliss DM, Wasserzug O. Incidence of retropharyngeal calcific tendinitis (longus colli tendinitis) in the general population. Otolaryngol Head Neck Surg. 2013;148(6):955-958.
doi pubmed - Chung T, Rebello R, Gooden EA. Retropharyngeal calcific tendinitis: case report and review of literature. Emerg Radiol. 2005;11(6):375-380.
doi pubmed - Hartley J. Acute Cervical Pain Associated with Retropharyngeal Calcium Deposit. A Case Report. J Bone Joint Surg Am. 1964;46:1753-1754.
pubmed - Ring D, Vaccaro AR, Scuderi G, Pathria MN, Garfin SR. Acute calcific retropharyngeal tendinitis. Clinical presentation and pathological characterization. J Bone Joint Surg Am. 1994;76(11):1636-1642.
pubmed - Offiah CE, Hall E. Acute calcific tendinitis of the longus colli muscle: spectrum of CT appearances and anatomical correlation. Br J Radiol. 2009;82(978):e117-121.
doi pubmed - Coulier B, Macsim M, Desgain O. Retropharyngeal calcific tendinitis—longus colli tendinitis—an unusual cause of acute dysphagia. Emerg Radiol. 2011;18(5):449-451.
doi pubmed - Razon RV, Nasir A, Wu GS, Soliman M, Trilling J. Retropharyngeal calcific tendonitis: report of two cases. J Am Board Fam Med. 2009;22(1):84-88.
doi pubmed - Kanzaria H, Stein JC. A severe sore throat in a middle-aged man: calcific tendonitis of the longus colli tendon. J Emerg Med. 2011;41(2):151-153.
doi pubmed - Haun CL. Retropharyngeal tendinitis. AJR Am J Roentgenol. 1978;130(6):1137-1140.
doi pubmed - Wolzak H, van de Rest M, Geurts M, Ter Borg EJ. Acute calcific tendinitis of the longus colli muscle: an often unrecognized cause of severe neck pain. J Clin Rheumatol. 2010;16(5):240-241.
doi pubmed - Paik NC, Lim CS, Jang HS. Tendinitis of longus colli: computed tomography, magnetic resonance imaging, and clinical spectra of 9 cases. J Comput Assist Tomogr. 2012;36(6):755-761.
doi pubmed
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Medical Cases is published by Elmer Press Inc.