

| Journal of Medical Cases, ISSN 1923-4155 print, 1923-4163 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Med Cases and Elmer Press Inc |
| Journal website http://www.journalmc.org |
Case Report
Volume 4, Number 10, October 2013, pages 676-678
Thenar Intramuscular Lipoma: A Case Report
Ivan Cherneva, b, c, Spencer Tingeyb
aWest Virginia School of Osteopathic Medicine, Lewisburg, West Virginia, USA
bBeckley Appalachian Regional Healthcare, Beckley, West Virginia, USA
cCorresponding author: Ivan Chernev, ARH Southern WV Clinic, 250 Stanaford Road, Beckley, WV, 25801, USA
Manuscript accepted for publication August 20, 2013
Short title: Thenar Intramuscular Lipoma
doi: https://doi.org/10.4021/jmc1474w
| Abstract | ▴Top |
Lipomas are one of the most common benign, mesenchymal neoplasms. They may be superficial or deep. Deep soft tissue lipomas of the hand are rare. Among them thenar intramuscular lipomas are very rare. We describe an unusual case of thenar intramuscular lipoma with its clinical and imaging characteristics.
Keywords: Lipoma; Intramuscular; Thenar
| Introduction | ▴Top |
Lipomas are one of the most common benign, mesenchymal neoplasms made up of mature adipose tissue [1]. They can be located anywhere in the body with the majority in the shoulder, back, head and neck. Soft tissue lipomas are divided into superficial and deep lesions. Most soft tissue lipomas are superficial and are located subcutaneously, whereas deep soft tissue lipomas present deep to the dermis under the investing fascia. Deep soft tissue lipomas are less common than superficial lipomas and can be located above muscle (supramuscular), below muscle (submuscular), between muscle (intermuscular), and within muscle (intramuscular) [2]. Thenar intramuscular lipomas are deep-seated soft tissue lipomas which are very rare. Only a few cases have been described in the English literature [3-5]. Herein, we report another case of thenar intramuscular lipoma with its clinical and imaging characteristics.
| Case Report | ▴Top |
An 87-year-old African-American woman presented to our office with a complaint of right hand thenar eminence mass first noted a few months ago. She reported mild discomfort in the area but otherwise full hand function. On physical examination, a mass was noted over the thenar eminence, which was soft on palpation (Fig. 1). The overlying skin was normal. There was no neurovascular compromise and strength was normal. Ultrasound (US) study showed an elongated, hyperechoic (compared to adjacent muscle), relatively well-defined mass with miniature hyperechoic lines (Fig. 2). Subsequent magnetic resonance imaging (MRI) revealed a bilobular high intensity signal mass with regions of ill-defined margins in the area of the thenar eminence suggestive of intramuscular lipoma (Fig. 3). The patient was referred to a hand surgeon. Excision of the lesion was performed under regional anesthesia. Intraoperatively, the thenar muscles were noted to be bulging above the mass. They were separated and the mass was excised completely. The mass measured 3.8 × 2.2 × 1.5 cm. Histologic diagnosis was lipoma with muscle cells at the edges of the mass. There was no evidence of malignancy. The patient had an uneventful postoperative period.
 Click for large image | Figure 1. Clinical photograph of the hand before surgery showing mass in the thenar eminence of the right hand. |
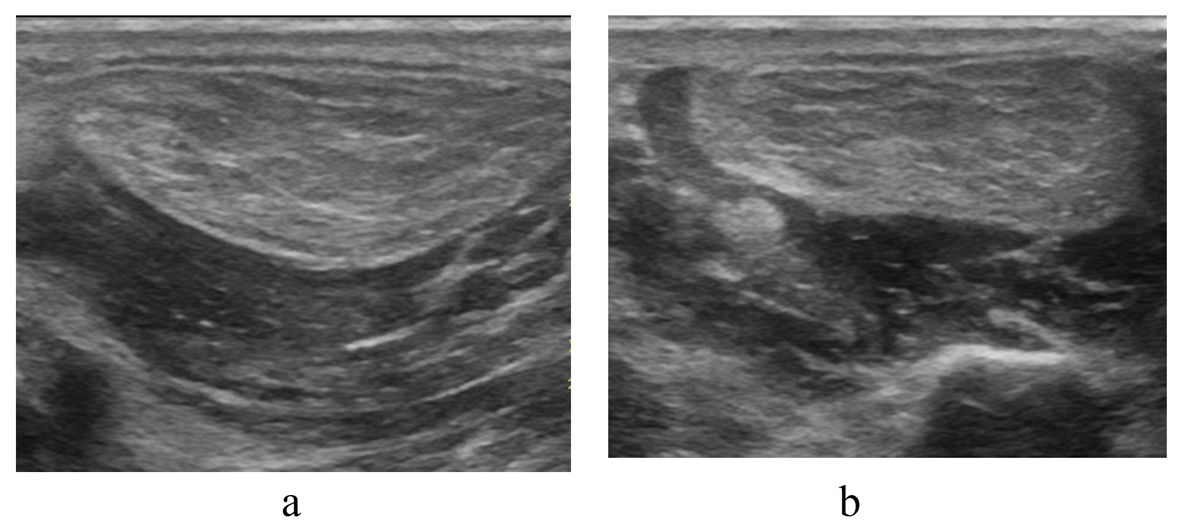 Click for large image | Figure 2. Thenar intramuscular lipoma. Longitudinal and transverse high-frequency US images showing hyperechoic (compared to adjacent muscle), relatively well-defined mass with miniature hyperechoic lines. |
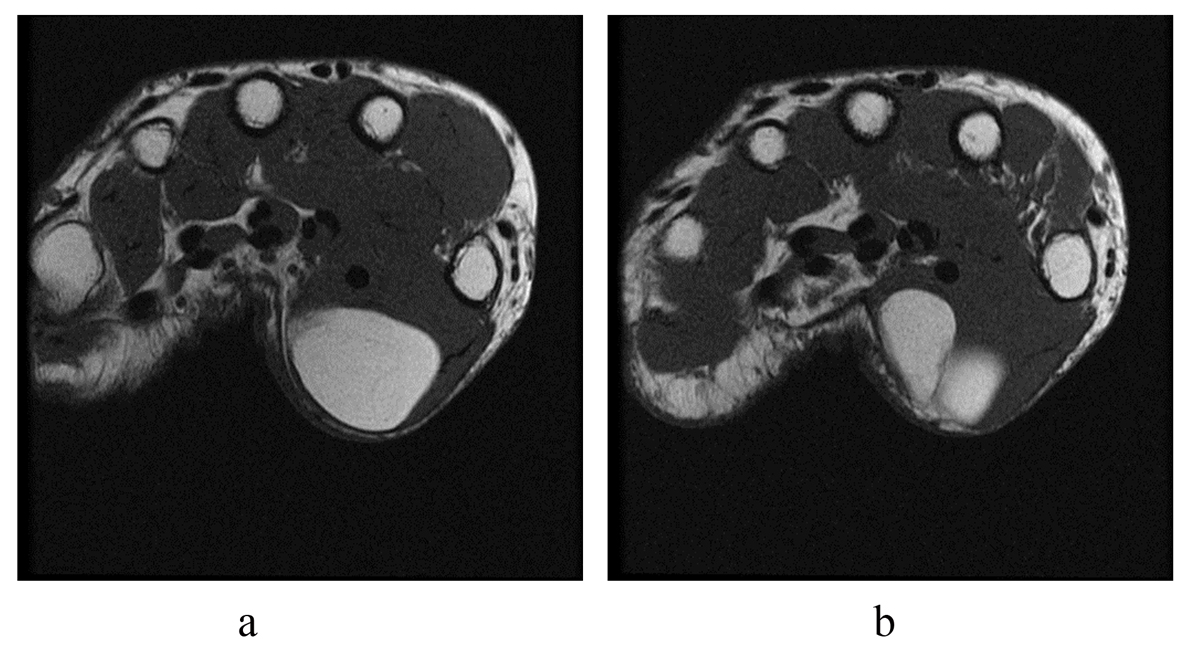 Click for large image | Figure 3. Thenar intramuscular lipoma. Two subsequent axial T1 MRI sections revealing bilobular high intensity signal mass with regions of ill-defined margins in the area of the thenar eminence. |
| Discussion | ▴Top |
Compared to superficial soft tissue lipomas, deep-seated soft tissue lipomas are less frequently encountered in clinical practice. Usually, they occur in the extremities and do not have as characteristic of clinical presentation as subcutaneous lipomas. They can grow around the muscles or can originate inside the muscle. Once they grow to a sufficient size they may involve both intramuscular and intermuscular tissues [5]. Intramuscular lipomas can be divided into two sub-groups: the infiltrative type and the well-circumscribed type. The infiltrative type is the more common of the two [3]. A lipoma of greater than 5 cm is classified as a “giant lipoma”. Larger lipomas may present with functional deficit or neurovascular compromise due to mass effect. Although the hand has an abundance of fat tissue, deep lipomas of the hand have been rarely described [3-8]. Thenar intramuscular lipoma is a very rare lesion which originates inside the thenar muscles. They will usually present with a slowly growing painless mass which may restrict range of motion. The overlying skin is normal and not adherent to the mass. Paresthesia due to compression of the radial digital nerve of the thumb has been described as a presenting symptom of thenar intramuscular lipomas as well [3].
Lipomas have been evaluated initially with US because of its availability and low cost compared to MRI. However, the sonographic features of lipomas have been shown to be variable. The echogenicity of lipomas may range from hypoechoic to hyperechoic depending on the degree of connective tissue and other reflective interfaces presented within the lipoma. The ultrasonographic definition of borders is also highly variable with different percentage of well-defined vs. ill-defined borders among different studies [1]. In a study of 39 soft-tissue masses (25 lipomas) Inampudi et al concluded that the variable sonographic appearance that is subjectively difficult to characterize accounts for the limitations of ultrasonography in accurately differentiating soft-tissue lipomas from other masses [1]. In a more recent study Paunipagar et al described the US features of deep-seated lipomas in a retrospective review of 64 lesions. They concluded that although the features of deep-seated lipomas are more variable than those reported for subcutaneous lipomas, the presence of internal echos in conjunction with other less specific features should enable a correct diagnosis [2]. However, none of their cases were located in the thenar muscles. Zamora et al described the ultrasound features of a single case of invasive thenar intramuscular lipoma. Initially, it was well-defined and hyperechoic compared to adjacent muscles and slightly inhomogenic. It was surgically removed but reoccurred 2.5 months later. Follow up US study showed infiltration of adjacent muscle by hyperechoic strands at the periphery of the mass [5]. Our case had hyperechoic appearance compared to adjacent muscles with relatively well-defined borders and no identifiable infiltration of adjacent muscles. Although ultrasound can be a valuable initial imaging study anatomical relations and full extent can be difficult to assess. In our case, we were not able to identify the two lobules on the ultrasound study, which were subsequently picked up on MRI (Fig. 3).
MRI is useful in distinguishing intramuscular lipomas from other soft tissue tumors. Matsumoto et al studied the MRI characteristics of intramuscular lipomas in a retrospective review of 17 consecutive cases [9]. They concluded that MRI findings of intramuscular lipomas varied from a small, single and homogeneous mass identical to ordinary (superficial) lipomas, to a large, inhomogeneous lesion with infiltrative margins. The presence of infiltrative margins and intermingled muscle fibers in intramuscular lipoma indicated a benign lesion rather than malignancy. In addition, uninodularity of the mass is helpful in differentiating intramuscular lipoma from well-differentiated liposarcoma. Our case showed a high-intensity, relatively homogeneous, bilobular mass with areas of ill-defined margins. Subsequent finding of muscle fibers at the edges of the tumor on histology confirmed the invasive nature of this intramuscular lipoma. As mentioned above, we were not able to identify both lobes on US examination. This reinforces the fact that if a deep lipomatous mass is found in the area of the hand follow up MRI is needed to delineate the extent of the mass and to look for other MRI findings to confirm the diagnosis.
Surgical excision is the treatment of choice for thenar intramuscular lipoma. In most reported cases, surgical excision of the lipoma resulted in full functional recovery. Due to its rarity however, the recurrence rate is unclear.
In conclusion, thenar intramuscular lipoma is a rare deep-seated lipoma. Certain US and MRI features may increase the accuracy of imaging diagnosis. Surgical excision is the definitive treatment although local recurrence is not uncommon especially in the infiltrative type.
Conflicts of Interest
The authors declare that there is no conflict of interests regarding the publication of this article.
| References | ▴Top |
- Inampudi P, Jacobson JA, Fessell DP, Carlos RC, Patel SV, Delaney-Sathy LO, van Holsbeeck MT. Soft-tissue lipomas: accuracy of sonography in diagnosis with pathologic correlation. Radiology. 2004;233(3):763-767.
doi pubmed - Paunipagar BK, Griffith JF, Rasalkar DD, Chow LT, Kumta SM, Ahuja A. Ultrasound features of deep-seated lipomas. Insights Imaging. 2010;1(3):149-153.
doi pubmed - Lee YH, Jung JM, Baek GH, Chung MS. Intramuscular lipoma in thenar or hypothenar muscles. Hand Surg. 2004;9(1):49-54.
doi pubmed - Mohan L, Semoes J. Thenar Intramuscular Lipoma: An Unusual Case. The Internet Journal of Surgery. 2008 Volume 17 Number 2.
- Zamora MA, Zamora CA, Samayoa EA, Morales HA, Ceballos JF. High-resolution ultrasonography in an aggressive thenar intramuscular lipoma. J Ultrasound Med. 2005;24(8):1151-1155.
pubmed - Kamath BJ, Kamath RK, Bhardwaj P, Shridhar, Sharma C. A Giant Lipoma In The Hand - Report Of A Rare Case. Online J Health Allied Scs.2006;1:6.
- Grivas TB, Psarakis SA, Kaspiris A, Liapi G. Giant lipoma of the thenar—case study and contemporary approach to its aetiopathogenicity. Hand (N Y). 2009;4(2):173-176.
doi pubmed - Pagonis T, Givissis P, Christodoulou A. Complications arising from a misdiagnosed giant lipoma of the hand and palm: a case report. J Med Case Rep. 2011;5(1):552.
doi pubmed - Matsumoto K, Hukuda S, Ishizawa M, Chano T, Okabe H. MRI findings in intramuscular lipomas. Skeletal Radiol. 1999;28(3):145-152.
doi pubmed
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Medical Cases is published by Elmer Press Inc.