

| Journal of Medical Cases, ISSN 1923-4155 print, 1923-4163 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Med Cases and Elmer Press Inc |
| Journal website http://www.journalmc.org |
Case Report
Volume 4, Number 7, July 2013, pages 488-490
A Rare Etiology of Acute Abdomen Syndrome: Gallbladder Torsion
Arslan Yusufa, Demir Hakana, d, Altintoprak Fatihb, Gunduz Yaseminc, Uzunoglu Yenera
aDepartment of General Surgery, Sakarya University Research and Educational Hospital, Sakarya, Turkey
bDepartment of General Surgery, Sakarya University Faculty of Medicine, Sakarya, Turkey
cDepartment of Radiology, Sakarya University Faculty of Medicine, Sakarya, Turkey
dCorresponding author: Demir Hakan, Sakarya University Research and Educational Hospital, Department of General Surgery, Sakarya, Turkey
Manuscript accepted for publication May 16, 2013
Short title: Gallbladder Torsion
doi: https://doi.org/10.4021/jmc1293e
| Abstract | ▴Top |
Acute abdomen syndrome is a frequently encountered clinical condition in emergency departments and includes a wide spectrum of surgical diagnoses. On the other hand, gallbladder torsion is a very rarely seen cause of the acute abdomen syndrome. A 74-year-old male patient admitted to the emergency department with abdominal pain present for two days, with gradually increasing intensity. Diffuse tenderness and guarding was present in the abdominal examination with positive Murphy sign. According to the radiologic evaluation, the patient was taken to the operation room under emergency condition with the preliminary diagnosis of gallbladder perforation. Total gallbladder necrosis due to torsion was detected in operation and cholecystectomy was performed. This case has been presented because of its rare incidence and emphasize that its preoperative diagnosis is very difficult.
Keywords: Perforation; Gallbladder torsion; Surgery; Acute abdomen syndrome
| Introduction | ▴Top |
Abdominal pain is one of the most frequently encountered complaints in emergency services with varying duration and severity. Although gallbladder pathologies are frequently encountered clinical situations worldwide, spontaneous perforation or necrosis of the gallbladder are very unusual compared to some other gallbladder conditions that might be managed non-operatively. Gallbladder torsion which has been first described in 1898, is an extremely rare surgical acute abdomen etiology [1]. Literature findings are generally limited to case reports of intra-operatively diagnosed cases. In this paper, diagnostic approaches and treatment result of a patient with gallbladder torsion are presented.
| Case Report | ▴Top |
A 74-year-old male patient admitted to the emergency department with progressively increasing abdominal pain of two days’ duration. His past medical history revealed a surgical operation for cancer of the larynx 18 years prior. Hemodynamic parameters of the patient with a tracheostomy were stable at admission (Blood pressure: 130/90 mmHg, pulse rate: 84 /min). He had no fever. Upon physical examination, diffuse tenderness and guarding in the abdomen, which was more marked in the right upper quadrant, was present with a palpable gallbladder in the right upper quadrant and a positive Murphy’s sign. Laboratory evaluations were within the normal range, other than leukocytosis (27,800 /mm3). Abdominal graphy examination was normal. Abdominal ultrasonography (USG) and computed tomography (CT) imaging revealed a hydropic gallbladder with a thickened wall (20 mm) and pericholecystic free-fluid, and its borders with the liver could not be defined clearly (Fig. 1, 2). Gallbladder perforation was considered as preliminary diagnosis. The decision to operate was made according to the physical examination, radiological findings, and presence of leukocytosis. Upon exploration of the abdomen, the gallbladder area was found to be severely inflamed with adhesions to surrounding tissues. The gallbladder was black in color, but there was no free bile in the abdomen. With continuing exploration, the gallbladder was found to have torsion of 180o along the axis of the cystic duct and artery. Necrosis had developed due to torsion, but no perforation was present (Fig. 3). The patient underwent a cholecystectomy with an uneventful postoperative course and was discharged on the second postoperative day. The patient was fine on the third month of follow-up.
 Click for large image | Figure 1. Abdomen USG; hydropic and lobulated gallbladder (arrow). |
 Click for large image | Figure 2. Abdomen CT; a hydropic gallbladder with a thickened wall (arrow) and pericholecystic free-fluid (double arrow). |
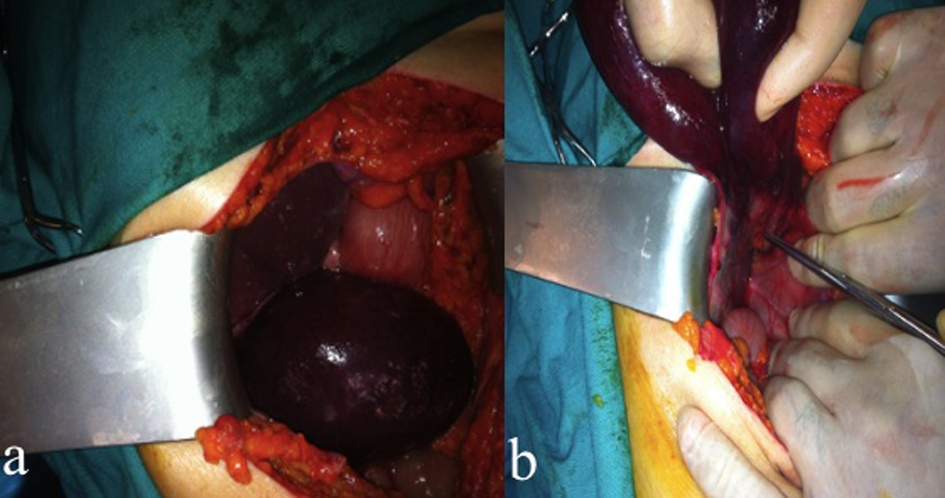 Click for large image | Figure 3. Operative findings; gallbladder necrosis view (a), and torsion of 180o along the axis of the cystic duct and artery (b). |
| Discussion | ▴Top |
Torsion of the gallbladder is quite a rare condition and the literature findings are limited to case reports. A common point in the reported cases is the presence of an anatomical attachment of a short segment of gallbladder to the liver or a completely separated gallbladder and liver, which merits the expression “floating gallbladder”. Liver atrophy and a loss of visceral fat with supportive tissue function are thought to cause this situation [2]. Inadequate fixation of the gallbladder to the liver results in excessive mobilization ability, which increases its chance of torsion. Although the peristaltic movements of the stomach and colon have also been blamed to cause gallbladder torsion, it is not yet clear which mechanism of movement may actually cause gallbladder torsion [3]. In the present case, the gallbladder was almost completely separated from the liver bed, and was able to freely rotate along its pedicle composed of the cystic artery and duct.
Gallbladder torsion is more frequent in the elderly and in females, although it can be seen in all age groups [4]. The main complaint is the sudden onset of severe abdominal pain, generally localized in the right upper quadrant; nausea and vomiting and fever may sometimes accompany this complaint. A common finding upon physical examination is a mass in the right upper quadrant of the abdomen. Our case presented with a severe sudden onset of right upper quadrant pain in accordance with the literature. Although there was no nausea or vomiting at presentation, a palpable mass was present on physical examination in the right upper quadrant.
Abdominal USG and CT findings in gallbladder torsion are a thickened gallbladder wall due to edema, a volume increase in the gallbladder lumen due to bile accumulation, necrosis in the gallbladder wall in the chronic phase, and pericholecystic fluid and free air when perforation is present [5]. Gallbladder blood flow can be examined in detail by Doppler USG, and a decreased or absent pericholecystic vascularity suggests torsion [6]. In the present case, the gallbladder was hydropic with an increased wall thickness and hypoechogenic submucosal layer. Gallbladder wall margins were obscured with condensed bile with linear echogenities seen in the lumen. These findings were consistent with acute cholecystitis. An abdomen CT revealed a severely hydropic gallbladder (11 × 9 × 7 cm) with a thickened wall (20 mm), pericholecystic free fluid, and increased density in the surrounding fatty tissue. Perforation of the gallbladder was assumed, according to the present findings.
Although various radiological signs have been defined in gallbladder torsion, preoperative diagnosis is extremely difficult. Surgical treatment, which is the only treatment option, usually serves as a diagnostic tool, as well. The choice of treatment is a cholecystectomy, which may be performed by open or laparoscopic methods [7]. Although it is very difficult to diagnose gallbladder torsion preoperatively, the possibility to encounter a technical problem during surgery is low, since the gallbladder is generally separated from the liver bed with a free pedicle in these cases, and can be mobilized easily. In this case, we did not think of gallbladder torsion preoperatively. We chose the option of open surgery since we thought to encounter a complicated clinical picture of gallbladder perforation or empyema, based on radiologic findings. During the operation, we discovered a floating gallbladder, and thus the procedure of cholecystectomy was completed easily without any complications.
In conclusion, torsion of the gallbladder is an extremely rare etiology of acute abdomen syndrome. Preoperative diagnosis necessitates advanced surgical and radiologic experience.
Conflict of Interest
None.
| References | ▴Top |
- Gupta V, Singh V, Sewkani A, Purohit D, Varshney R, Varshney S. Torsion of gall bladder, a rare entity: a case report and review article. Cases J. 2009;2:193.
doi pubmed - Janakan G, Ayantunde AA, Hoque H. Acute gallbladder torsion: an unexpected intraoperative finding. World J Emerg Surg. 2008;3:9.
doi pubmed - Losken A, Wilson BW, Sherman R. Torsion of the gallbladder: a case report and review of the literature. Am Surg. 1997;63(11):975-978.
pubmed - Tarhan OR, Barut I, Dinelek H. Gallbladder volvulus: review of the literature and report of a case. Turk J Gastroenterol. 2006;17(3):209-211.
pubmed - Tajima Y, Tsuneoka N, Kuroki T, Kanematsu T. Clinical images. Gallbladder torsion showing a "whirl sign" on a multidetector computed tomography scan. Am J Surg. 2009;197(1):e9-10.
doi pubmed - Boer J, Boerma D, de Vries Reilingh TS. A gallbladder torsion presenting as acute cholecystitis in an elderly woman: A case report. J Med Case Rep. 2011;5(1):588.
doi pubmed - Boonstra EA, van Etten B, Prins TR, Sieders E, van Leeuwen BL. Torsion of the gallbladder. J Gastrointest Surg. 2012;16(4):882-884.
doi pubmed
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Medical Cases is published by Elmer Press Inc.