

| Journal of Medical Cases, ISSN 1923-4155 print, 1923-4163 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Med Cases and Elmer Press Inc |
| Journal website http://www.journalmc.org |
Case Report
Volume 4, Number 2, February 2013, pages 114-115
The Discovery of a Choledochal Cyst During a Single-Port Cholecystectomy With Intra-Operative Cholangiogram
Andrea Rossettia, b, Pascal Buchera, Nicolas Christian Buchsa, Philippe Morela, Christian Tosoa
aDepartment of Visceral Surgery and Transplantation, Geneva University Hospital, Kantonspital St. Gallen, Clinic of Surgery, Switzerland
bCorresponding author: Andrea Rossetti, Clinic of Surgery, Kantonspital St. Gallen, Roscharcherstrasse 95 St. Gallen 9007, Switzerland
Manuscript accepted for publication November 12, 2012
Short title: Discovery of Choledochal Cyst
doi: https://doi.org/10.4021/jmc1011e
| Abstract | ▴Top |
Choledochal cyst is a rare congenital malformation, which is most often discovered in pediatric patients. Perioperative cholangiography is routinely performed in our institution during standard or single-port cholecystectomies. We report the case of a 25 year-old woman with a choledochal cyst identified during a single-port cholecystectomy with cholangiogram. The case illustrates the feasibility and usefulness of single-port intra-operative cholangiogram.
Keywords: Single site laparoscopic surgery; Cholecistectomy; SILS
| Introduction | ▴Top |
Choledochal cysts (CCs) are the most frequent malformations of the extrahepatic bile duct, but remain extremely rare with an estimated yearly incidence of 0.5/million. About 3,000 cases have been reported in the literature thus far, with a higher female prevalence (female/male: 3/1) [1-3].
The pathogenesis of CCs remains unclear, but may be related to an abnormal pancreaticobiliary duct junction, leading to a chronic inflammation and damages to the duct wall [4]. The initial investigation of the bile duct tree should include an ultrasound. Subsequently, a CT scan, ERCP and/or MRCP can help better understand the anatomy [5].
In some patients, the cyst remains asymptomatic and can be discovered during investigations performed for other reasons or during surgery. We illustrate this possibility by reporting the case of a patient with a CC discovered during a single-port cholecystectomy with cholangiogram. We also discuss the usefulness and safety of single-port cholangiogram.
| Case Report | ▴Top |
A 25-year-old woman with symptomatic cholelithiasis has been admitted for an elective cholecystectomy. An abdominal ultrasound has been performed and revealed gallstones without signs of inflammation or abnormality of the bile duct anatomy. Liver function tests were normal.
A single-port cholecystectomy has been performed with cholangiogram. A clip was placed proximally on the cystic duct, a small incision made and a cholangiography catheter (Cook™ type) inserted. The cholangiogram images were further acquired similar to the standard procedure [6] and a large CC with a dilated intrahepatic bile duct was discovered (Fig. 1). The cholecystectomy was successfully completed and the patient discharged within 24 hours.
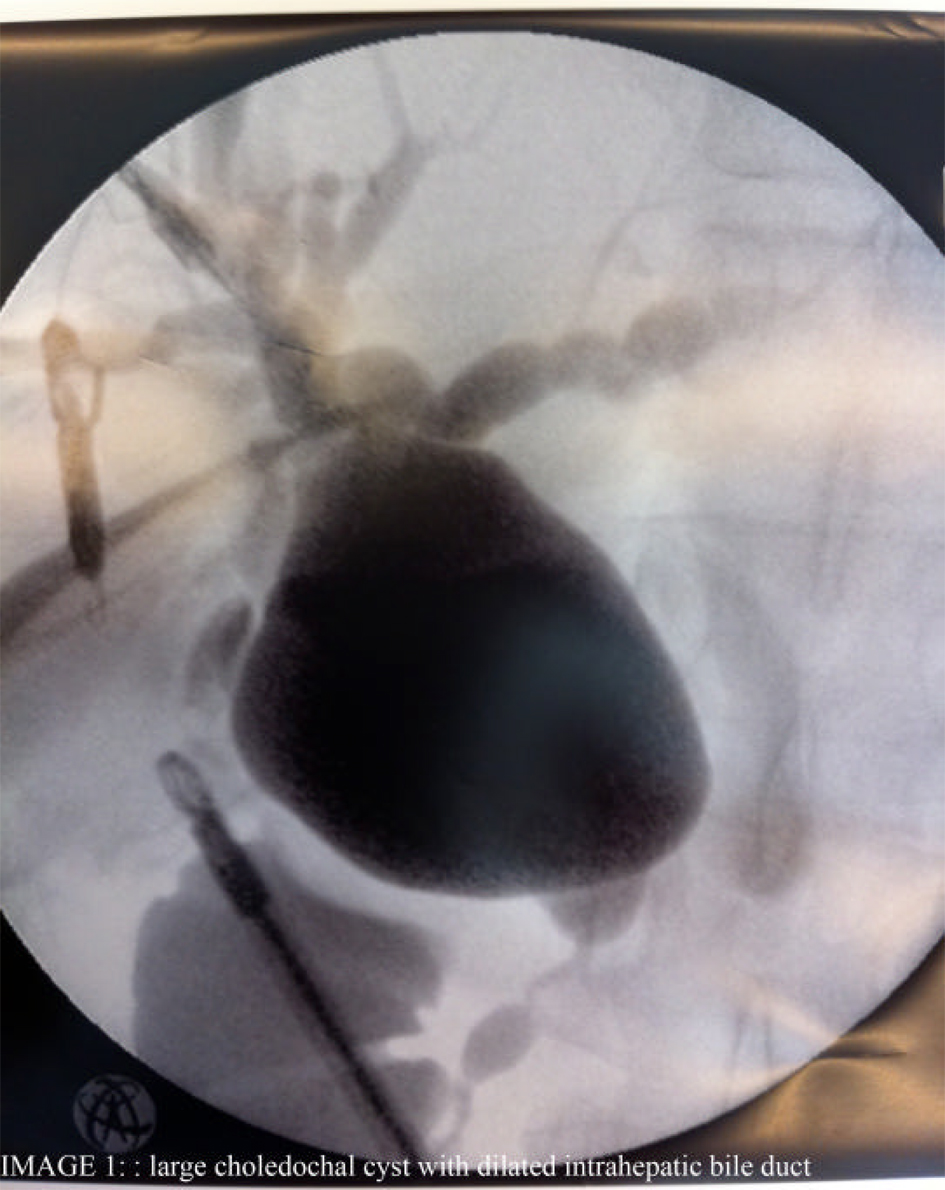 Click for large image | Figure 1. Large choledochal cyst with dilated intrahepatic bile duct. |
Due to the presence of a dilated intrahepatic bile duct and the risk of cancer degeneration, the patient has been suggested to undergo the resection of the cyst and the extrahepatic bile duct with choledoco-jejunostomy. While being non symptomatic, she declined the offered management.
| Discussion | ▴Top |
Intraoperative cholangiogram can be very useful for the detection of common bile duct stone, a better assessment of the bile duct anatomy and a safer dissection with lower rates of bile duct injury during cholecystectomy [7, 8]. In addition, it can help detecting bile duct injury earlier. Based on these observations and in order to improve safety, our institutional policy includes an intraoperative cholangiogram for all cholecystectomies, whether standard or single-port. Of note, while more difficult during single-port procedures, a cholangiogram was successfully performed in 87% out of 175 consecutive single-port cholecystectomies [9].
The case reported herein further illustrates the usefulness of this strategy in a patient undergoing single-port cholecystectomy. While the patient was non symptomatic, the intraoperative cholangiogram was the best way to detect and characterize the described CC. While rare, the detection of CC is critical as it is linked to a significant risk of malignant degeneration [10-11]]. A review of 73 Japanese institutions has identified 154 cases of malignancy in 881 patients with choledochal cysts (prevalence of 17%) [12].
Conclusion
The present report illustrates the feasibility and usefulness of intraoperative cholangiogram during single-port cholecystectomy. We would suggest performing cholangiogram in all patients (or at least with low threshold) even during single-port surgery.
| References | ▴Top |
- Savic D, Milovanovic D, Jovanovic D. [Congenital dilatation of the common bile duct (congenital choledochal cyst)]. Srp Arh Celok Lek. 2001;129(Suppl 1):47-50.
- O'Neill JA, Jr., Templeton JM, Jr., Schnaufer L, Bishop HC, Ziegler MM, Ross AJ, 3rd. Recent experience with choledochal cyst. Ann Surg. 1987;205(5):533-540.
doi pubmed - Tan KC, Howard ER. Choledochal cyst: a 14-year surgical experience with 36 patients. Br J Surg. 1988;75(9):892-895.
doi - Babbitt DP. [Congenital choledochal cysts: new etiological concept based on anomalous relationships of the common bile duct and pancreatic bulb]. Ann Radiol (Paris). 1969;12(3):231-240.
- Singham J, Yoshida EM, Scudamore CH. Choledochal cysts: part 2 of 3: Diagnosis. Can J Surg. 2009;52(6):506-511.
pubmed - Bucher P, Buchs N, Pugin F, Ostermann S, Morel P. Single port access laparoscopic cholecystectomy (with video): reply. World J Surg. 2011;35(5):1150-1151.
doi pubmed - Singham J, Yoshida EM, Scudamore CH. Choledochal cysts. Part 3 of 3: management. Can J Surg. 2010;53(1):51-56.
pubmed - Araujo Neto NP, Goncalves JE, Bromberg SH, Guz B, Zanoto A. Predicao da coledocolitiase pela associacao de indicadores clinicos e laboratoriais em dois momentos do pre-operatorio dacolecistectomia. Rev Col Bras Cir. 2005;32(1):41-46.
doi - Bucher P, Morel P. Development of laparoscopic single-site cholecystectomy mandates critical view of safety dissection and routine intraoperative cholangiography. J Am Coll Surg. 2011;212(3):422-423; author reply 423.
doi pubmed - Saad N, Darcy M. Iatrogenic bile duct injury during laparoscopic cholecystectomy. Tech Vasc Interv Radiol. 2008;11(2):102-110.
doi pubmed - West J, Wood H, Logan RF, Quinn M, Aithal GP. Trends in the incidence of primary liver and biliary tract cancers in England and Wales 1971-2001. Br J Cancer. 2006;94(11):1751-1758.
doi pubmed - Watanabe Y, Toki A, Todani T. Bile duct cancer developed after cyst excision for choledochal cyst. J Hepatobiliary Pancreat Surg. 1999;6(3):207-212.
doi pubmed
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Medical Cases is published by Elmer Press Inc.