

| Journal of Medical Cases, ISSN 1923-4155 print, 1923-4163 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Med Cases and Elmer Press Inc |
| Journal website http://www.journalmc.org |
Case Report
Volume 2, Number 6, December 2011, pages 287-288
Varicella Zoster Myopericarditis
Muhammet Rasit Sayina, b, Turgut Karabaga, Oguzhan Celika, Mehmet Ali Cetinera, Cem Cila, Mustafa Aydina
aZonguldak Karaelmas University, School of Medicine, Department of Cardiology, Kozlu 67600, Zonguldak, Turkey
bCorresponding author: Muhammet Rasit Sayin, Zonguldak Karaelmas University, School of Medicine, Department of Cardiology, Kozlu 67600, Zonguldak, Turkey
Manuscript accepted for publication October 21, 2011
Short title: Varicella Zoster Myopericarditis
doi: https://doi.org/10.4021/jmc398w
| Abstract | ▴Top |
Varicella zoster virus infections are common in children and most recover without complication. Myopericarditis is an uncommon but serious complication of varicella zoster virus infection and may lead to severe morbidity and mortality. Myopericarditis can be very similar to acute myocardial infarction at presentation and therefore may have result with thrombolytic mistreatment. We report a case with chickenpox myopericarditis suggestive of acute myocardial infarction.
Keywords: Varicella zoster; Myocarditis; Pericarditis
| Introduction | ▴Top |
Typical chest pain, ST segment elevation and elevated troponin levels resemble acute myocardial infarction (AMI). Myopericarditis can be very similar to AMI at presentation and therefore may have result with thrombolytic mistreatment. Myopericarditis is a rare but serious complication of varicella zoster virus (VZV) infection (chichenpox). We report a case with chickenpox myopericarditis suggestive of AMI.
| Case Report | ▴Top |
A 16-year-old male patient was admitted to our emergency service with a suspect of acute coronary syndrome. He had severe chest pain which continued 20 minutes and regressed three hours ago before presentation. The chest pain was constant and radiated to his left arm. He did not have any cardiac risk factors. Previously he had experienced no major illness.
Physical examination revealed blood pressure of 120/80 mmHg, heart rate of 78 bpm and normal cardiorespiratory findings. There was papulomaculoid exanthema on his face, scalp and body consistent with a chickenpox infection (Fig. 1). The resting electrocardiography (ECG) showed regular sinus rhythm; 0.3 mV ST elevation in lead DII; 0.2 mV ST elevation in leads DIII, aVF, V5-6 (Fig. 2). Laboratory tests revealed a creatine kinase (CK) of 1828.8 U/L (26-174 U/ L), mass CK-MB of 28.7 ng/ml (0.6-6.3 ng/ml), Troponin T of 3.35 ng/ml (<0.01 ng/ml), and C-reactive protein of 31.2 mg/l (2-5 mg/l). Chest X-ray was normal. Echocardiograpy showed normal findings except minimal pericardial effusion at the basal of the right atrium. The diagnosis of chickenpox was confirmed by the finding of a raised immunoglobulin M against varicella zoster on enzymelinked immunosorbent assay. Final diagnosis was varicella zoster myopericarditis.
 Click for large image | Figure 1. Papulomaculoid exanthema |
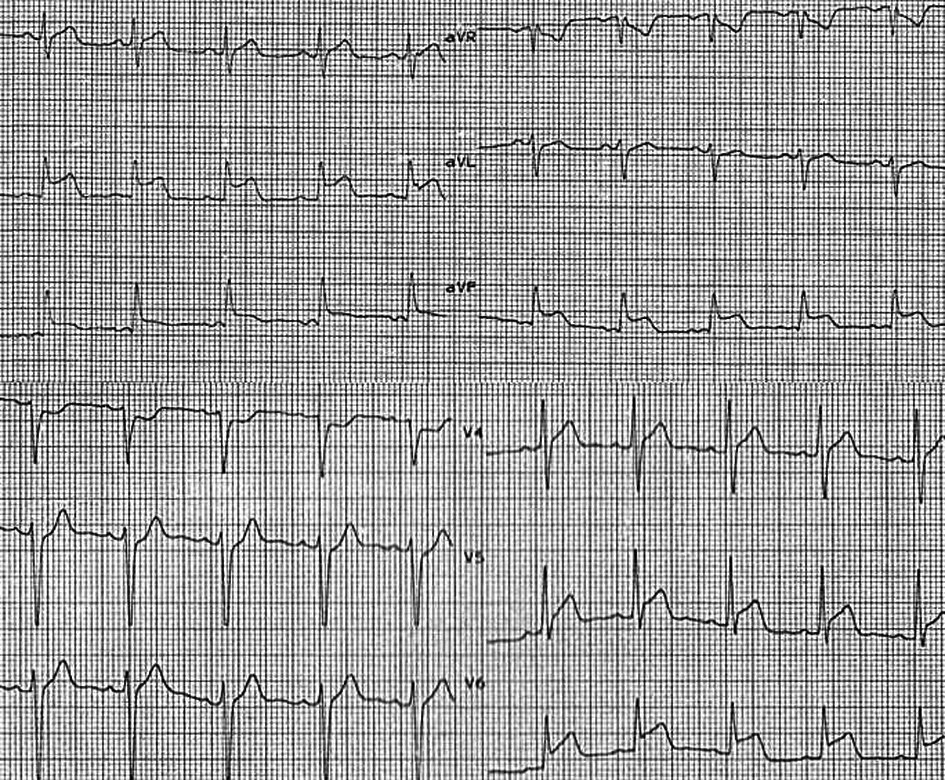 Click for large image | Figure 2. ECG |
The patient was treated with ibuprofen (2 x 600mg). Echocardiograpy at 2 weeks confirmed normal cardiac functions with no pericardial effusion.
| Discussion | ▴Top |
VZV is one of the most common infectious agents to affect respiratory system. VZV infections are common in children and most recover without complication. Serious complications are rare but may be life threatening, including bacterial superinfection, Reye’s syndrome, encephalitis, and pneumonia [1]. However, VZV is a cardiotrophic virus. Myopericarditis is also an uncommon but serious complication of VZV infection and may lead to severe morbidity and mortality. Myocarditis following varicella was first described by Hackel in 1953 [2]. Since then there have been several published reports of myocarditis or pericarditis caused by VZV. Patients may present with heart failure which may lead to cardiac transplantation [3] or normal cardiac functions as in our case. The ECG in our case, which revealed ST segment elevations in leads DII, DIII, aVF and V5-6, is not typically for pericarditis and may be results acute myocardial infarction misdiagnosis. Typical pericarditis ECG shows ST segment elevations and PR segment depressions in all leads without aVR and V1. Although the symptoms and signs of varicella myopericarditis vary, the presentation in our case, including chest pain, ST segment elevation and elevated troponin levels, is the same as in patients with AMI and may produce dangerous outcomes because of thrombolytic treatment.
Most cases need only supportive treatment, but some cases might require antiviral agents, immunoglobulin, a pacemaker, extracorporeal membrane oxygenation, or cardiac transplantation [3, 4]. Because of life threatening conditions, patients with VZV infection and cardiac symptoms should be investigated for possible myopericarditis.
| References | ▴Top |
- Jackson MA, Burry VF, Olson LC. Complications of varicella requiring hospitalization in previously healthy children. Pediatr Infect Dis J. 1992;11(6):441-445.
pubmed doi - Hackel DB. Myocarditis in association with varicella. Am J Pathol. 1953;29(3):369-379.
pubmed - Tsintsof A, Delprado WJ, Keogh AM. Varicella zoster myocarditis progressing to cardiomyopathy and cardiac transplantation. Br Heart J. 1993;70(1):93-95.
pubmed doi - Rich R, McErlean M. Complete heart block in a child with varicella. Am J Emerg Med. 1993;11(6):602-605.
pubmed doi
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Medical Cases is published by Elmer Press Inc.