

| Journal of Medical Cases, ISSN 1923-4155 print, 1923-4163 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Med Cases and Elmer Press Inc |
| Journal website http://www.journalmc.org |
Case Report
Volume 10, Number 2, February 2019, pages 46-48
Nodular Pulmonary Sarcoidosis
Mohammed Abdallaa, c, Wiam Mohamedb, Abdelnasir Mohameda, Cristina Corsinia
aPresence Saint Francis Hospital, Evanston, IL, USA
bUniversity of Khartoum, Khartoum, Sudan
cCorresponding Author: Mohammed Abdalla, Presence Saint Francis Hospital, Evanston, IL 60202, USA
Manuscript submitted January 1, 2019, accepted January 14, 2019
Short title: Nodular Pulmonary Sarcoidosis
doi: https://doi.org/10.14740/jmc3246
| Abstract | ▴Top |
Nodular sarcoidosis is a rare form of pulmonary sarcoidosis comprising 4% of lung involvement in this disease. It usually affects African American women with a mean age of 35 years. It presents with constitutional symptoms associated with chest imaging findings of multiple or solitary lung nodules. In our case we present a 38-year-old woman who had chronic productive cough associated with fever and dyspnea for 1 month. She had course of antibiotics without improvement in her symptoms. Chest imaging showed multiple nodules measuring up to 7.5 cm in size. Lung biopsy was obtained and histopathology revealed non-caseating granulomas consistent with sarcoidosis. Angiotensin-converting enzyme levels were elevated. She received systemic steroids and the nodules resolved on follow-up imaging.
Keywords: Sarcoidosis; Lung nodules; Nodular sarcoidosis
| Introduction | ▴Top |
Sarcoidosis is a disease of unknown etiology that is characterized by non-caseating granulomas in multiple organs. It can involve the lung in various forms. Nodular involvement is a rare form of pulmonary sarcoidosis which can be mistaken for malignancy. Diagnosis requires compatible clinical picture along with imaging findings suggestive of the disease and non-caseating granulomas on histopathology.
| Case Report | ▴Top |
A 38-year-old woman presented to the hospital with 1-month history of cough and shortness of breath, and the cough is productive of thick yellow sputum, associated with subjective fever and dyspnea on exertion. She also reports fatigue. She denies chest pain, hemoptysis, joint pain, eye pain, abdominal pain or leg swelling. She is a smoker and works as a housekeeper in a hotel. She emigrated from West Africa 15 years ago but denies recent travel or tuberculosis exposure. She keeps no pets at home.
Physical examination showed normal vital signs, and chest and cardiovascular exams were unremarkable. Lab investigations including complete blood count and comprehensive metabolic panel were unremarkable. Chest X-ray showed diffuse airspace opacities with peripheral distribution (Fig. 1). The patient was started on ceftriaxone and azithromycin for treatment of presumable community-acquired pneumonia. Despite treatment with antibiotics, the patient’s condition did not improve significantly. Pro-calcitonin was measured and levels were normal, and workup for fungal infection was negative. She underwent a chest computed tomography (CT) scan with contrast that revealed extensive multifocal bilateral airspace opacities with significant hilar and mediastinal lymphadenopathy (Figs. 2, 3). Given the lack of improvement in clinical picture, the decision was made to obtain a lung biopsy. Cultures of the biopsy were negative. Histopathology of the lung biopsy showed non-caseating granulomas, consistent with sarcoidosis. Angiotensin-converting enzyme levels were elevated. The patient was started on steroids and her condition improved clinically and on radiological imaging.
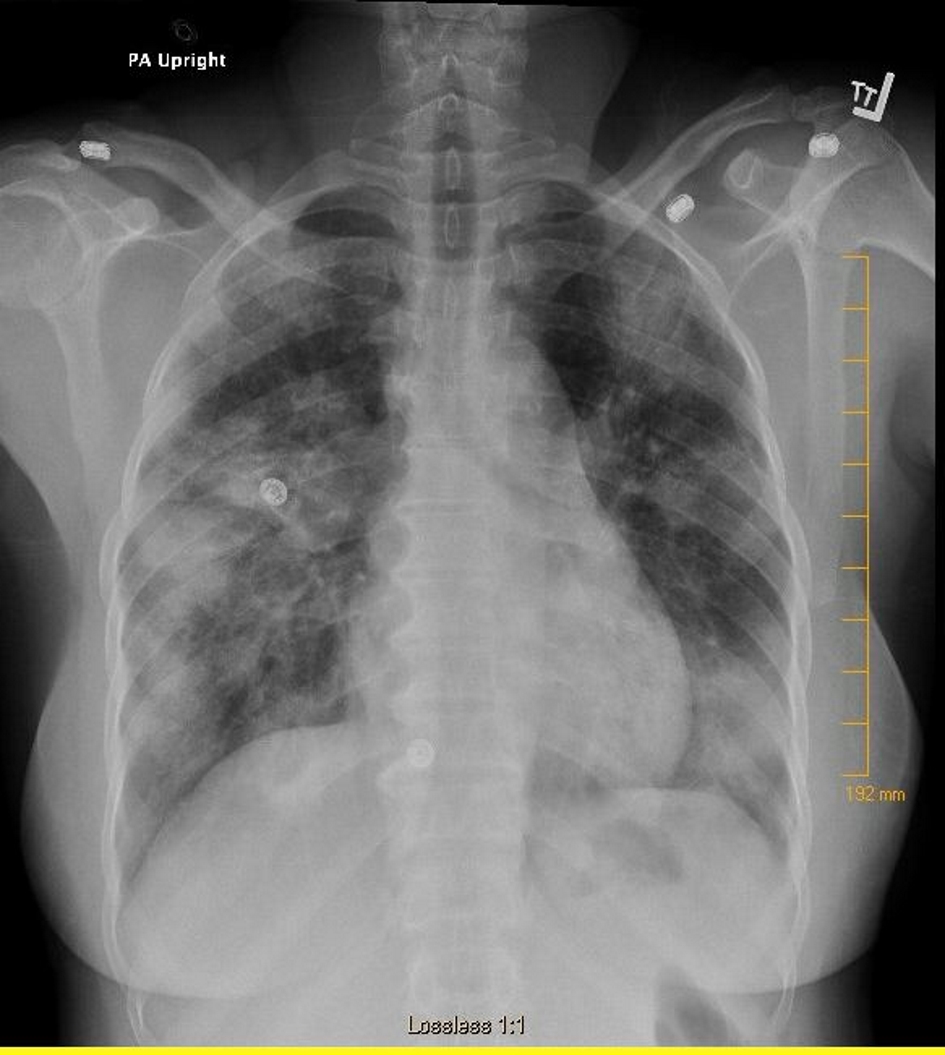 Click for large image | Figure 1. Chest X-ray showing multiple bilateral nodular opacities. |
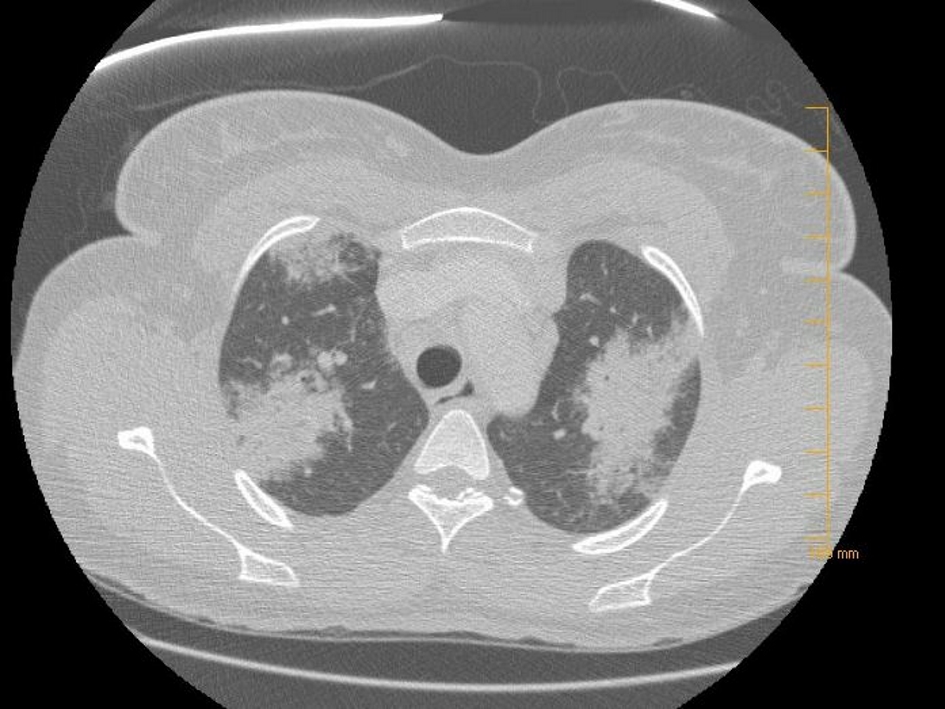 Click for large image | Figure 2. CT of the chest demonstrating multiple lung nodules on both sides of the chest. |
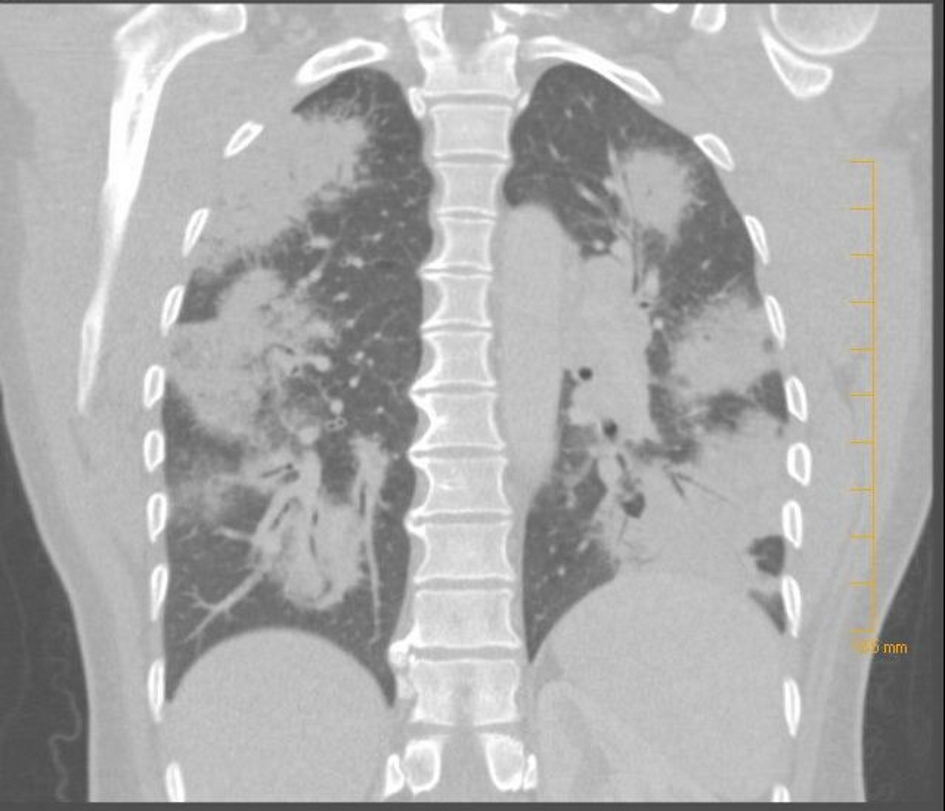 Click for large image | Figure 3. CT of the chest (coronal view) showing bilateral nodular lung involvement. |
| Discussion | ▴Top |
Sarcoidosis is a granulomatous disease that affects multiple organ systems, and the lung is the most commonly affected organ. Ungprasert et al showed equal involvement for men and women with a median age at diagnosis of 42 and 48 years, respectively. Intrathoracic involvement was demonstrated in 97% of patients affected with sarcoidosis [1]. Pulmonary involvement can be in forms of hilar and mediastinal lymphadenopathy, ground glass opacities, bronchial wall thickening, lung fibrosis, or nodular masses. In our report we present a case of nodular sarcoidosis which is a rare form comprising 2.4-4% of sarcoid lung involvement [2, 3].
Nodular sarcoidosis was described mainly in African American patients, with more women being affected than men, and the mean age is 35 as described by Malaisamy et al [4]. These nodules form as a result of coalescence of multiple granulomas to form masses up to 5 cm in size [5]. In our case report, the chest CT scan revealed multiple nodules measuring up to 7.5 cm. Patients with nodular sarcoidosis can present with fever, fatigue, weight loss and chronic cough. A study by Abehsera et al to correlate CT scan patterns of sarcoidosis with pulmonary function found that nodular sarcoidosis results in minimal functional impairment [6].
CT of the chest can demonstrate multiple lung nodules or solitary nodules. These lesions tend to be peripheral, predominantly involving the upper lobes and associated with lymphadenopathy [4]. Histopathology is crucial for the diagnosis, and it demonstrates non-caseating granulomas.
Nodular sarcoidosis has favorable prognosis with resolution of radiographic lesions and improvement of clinical picture either with systemic steroids or spontaneously [7]. Our patient received oral steroids for 2 months and follow-up imaging showed resolution of the lung lesions (Fig. 4).
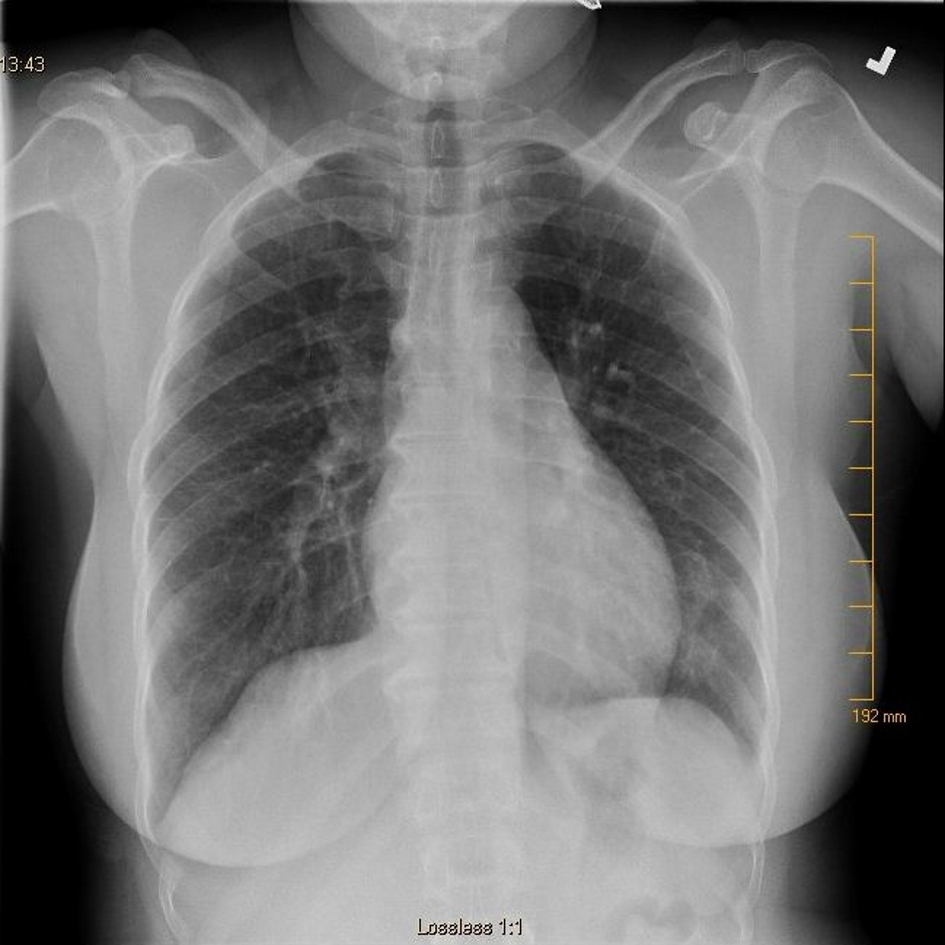 Click for large image | Figure 4. Chest X-ray showing resolution of the nodules after initiation of systemic steroids. |
| References | ▴Top |
- Ungprasert P, Crowson CS, Matteson EL. Influence of gender on epidemiology and clinical manifestations of sarcoidosis: a population-based retrospective cohort study 1976-2013. Lung. 2017;195(1):87-91.
doi pubmed - Sharma OP, Hewlett R, Gordonson J. Nodular sarcoidosis: an unusual radiographic appearance. Chest. 1973;64(2):189-192.
doi pubmed - Hansell DM AP, Lynch DA, Mc Adams HP. Imaging of diseases of the chest. 4. Philadelphia: Mosby; 2005. Miscellaneous lung diseases: sarcoidosis.
- Malaisamy S, Dalal B, Bimenyuy C, Soubani AO. The clinical and radiologic features of nodular pulmonary sarcoidosis. Lung. 2009;187(1):9-15.
doi pubmed - Ma Y, Gal A, Koss MN. The pathology of pulmonary sarcoidosis: update. Semin Diagn Pathol. 2007;24(3):150-161.
doi pubmed - Abehsera M, Valeyre D, Grenier P, Jaillet H, Battesti JP, Brauner MW. Sarcoidosis with pulmonary fibrosis: CT patterns and correlation with pulmonary function. AJR Am J Roentgenol. 2000;174(6):1751-1757.
doi pubmed - Shahzad H, Ur-Rehman S, Fatima K, Sharif N, Zubairi AB. Case series and literature review of multiple nodular sarcoidosis. BMC Res Notes. 2013;6:394.
doi pubmed
This article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Medical Cases is published by Elmer Press Inc.