

| Journal of Medical Cases, ISSN 1923-4155 print, 1923-4163 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Med Cases and Elmer Press Inc |
| Journal website http://www.journalmc.org |
Case Report
Volume 9, Number 12, December 2018, pages 403-405
Extramandibular Presentation in the Course of the Inferior Alveolar Nerve: A Case Report and Review of the Literature
Ilson Sepulvedaa, b, c, d, h, J. Patricio Ulload, e, Francisco Rivas-Rodriguezf, Rodrigo Barrosg
aSchool of Dentistry, Finis Terrae University, Concepcion, Chile
bRadiology Department, ENT-Head and Neck Surgery, Concepcion, Chile
cDental-Maxillofacial and Nuclear Medicine Services, General Hospital of Concepcion, Concepcion, Chile
dENT-Head and Neck Surgery Service, General Hospital of Concepcion, Concepcion, Chile
eUniversity of Concepcion School of Medicine, Concepcion, Chile
fDivision of Neuroradiology, Radiology Department, University of Michigan Health System, Ann Arbor, MI 48109, USA
gEmergency and Internal Medicine Services, General Hospital of Concepcion, Concepcion, Chile
hCorresponding Author: Ilson Sepulveda, ENT-Head and Neck Surgery Service, General Hospital of Concepcion, San Martin Av. 1436, Concepcion, Chile
Manuscript submitted November 13, 2018, accepted November 21, 2018
Short title: Extramandibular Submucosal Course of IAN
doi: https://doi.org/10.14740/jmc3215
| Abstract | ▴Top |
The inferior alveolar nerve (IAN) is a branch of the mandibular nerve, the third division of the trigeminal nerve (V cranial nerve). Its location and course into the mandible is very important because of its susceptibility to the injury during any surgical or prosthetic approaches. Cone beam computed tomography (CBCT) is a three-dimensional imaging modality, with less exposure than multi slice computed tomography (MSCT), being considered an ideal imaging tool for maxillofacial diagnosis. We present an unusual extramandibular submucosal course of IAN in relationship with a mandibular exostosis, and with no association with the sensory disorder.
Keywords: Atrophic; Mandible; Exostosis; Incidental finding; Cone beam computed tomography
| Introduction | ▴Top |
The inferior alveolar nerve (IAN) enters to the mandible by the mandibular foramen, located on medial aspect of the ramus, and runs in anterior and lateral direction inside the mandibular body, until exits by the mental foramen at the premolar region. In this course, it gives sensory nerves from incisive (through incisive nerve) to molar region, including to the mentolabial area. The knowledge of its considerable variation in the course, shape, curve, and directions is essential at moment to any surgical procedure plan in this area. Cone beam computed tomography (CBCT) provides an accurate location, and to determine any anatomical variation in the course of the mandibular canal and its relation with neighbor anatomical structures [1, 2].
| Case Report | ▴Top |
A 75-years-old female without a significant medical history, presented for imaging study of swelling on the medial aspect of the right mandibular body. The clinical exam revealed total edentulous jaw and hard swelling in the area mentioned above, without ulceration, pain or paresthesia. No other injuries or cervical lymphadenopathy were identified. Also, the patient presented no other symptoms.
CBCT was performed showing a hyperdense exostosis of the cortical bone without compromise of the bone marrow. As incidental finding demonstrated the entry and exit of the IAN canal in relationship with the exostosis (Fig. 1a, b), the volume rendering with virtual representation of the IAN confirmed this finding (Fig. 1c, d).
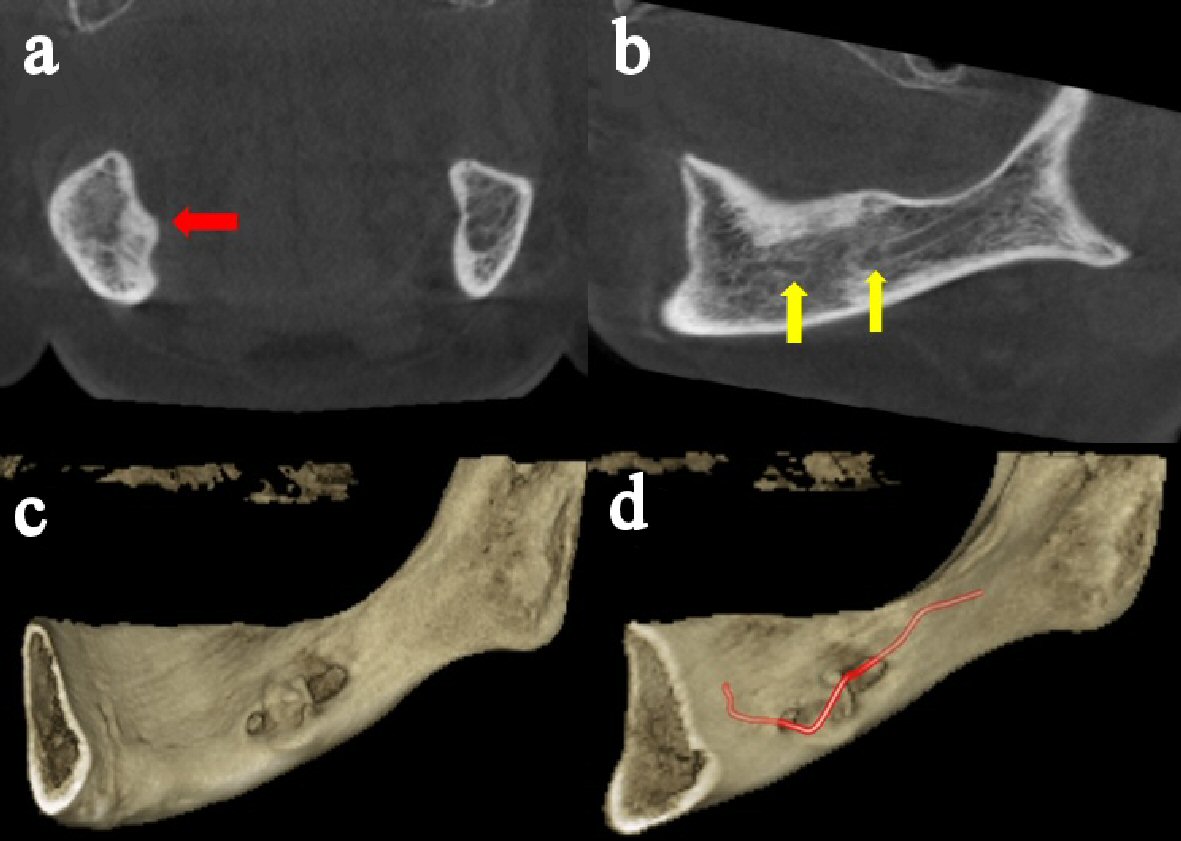 Click for large image | Figure 1. CBCT of the mandible shows a cortical bone exostosis in medial aspect of the right mandibular body (red arrow), exit and entry holes of the mandibular canal (yellow arrows). As shown the three- dimensional IAN course representation (red). (a) Coronal. (b) Oblique sagittal. (c, d) Osseous volume rendering. |
| Discussion | ▴Top |
IAN located outside of the mandible is a rare condition; it’s the most common presentation which is associated to severe atrophy in edentulous mandibles or hypoplastic condition in dentulous mandible [1]. Various imaging modalities including the conventional and computerized tomography have been used to evaluate mandibular morphology before a surgical procedure. In CBCT the appearance of the mandibular canal usually is a well-defined hypodense zone, lined by hyperdense borders [2].
From its origin, IAN runs obliquely down and forward, enters the medial mandibular ramus through the mandibular foramen; runs more or less horizontal, and ends between the apices of the first and second premolar, exiting the mental foramen giving terminal mental and incisive nerves [3].
Worthington described that there are three different configurations of the inferior alveolar canal (IAC) as follows: 1) A progressive curve rising from anterior to posterior; 2) A steep ascent from anterior to posterior; and 3) A catenary-like canal [4].
Sanam M. et al evaluated the IAN course in three age groups and demonstrated that straight and progressive descending pattern were the most prevalent pattern in the 20 - 29 years age group. In the 30 - 44 and 45 - 59 years age group the most prevalent category was recorded as straight and catenary, respectively, without any statistically significant difference between the three age groups [5].
Therefore, information on the buccolingual, superior and inferior position of the canal could assist surgeons in avoiding injury to the IAN [6]. Atieh Safaee et al established that the greatest distance, from IAC to the buccal cortex existed at the second molar region, where the lingual distances in some cases reached zero [7]. In the vertical dimension, A. Ozturk et al demonstrated that on average, the IAC rans almost 1 cm (range 6.10 - 15.30 mm) above the inferior border of the body of the mandible in the molar region [8].
Extracanalicular variations of the IAN are exceedingly rare and unreported. R. Manikandhan et al reported absent mandibular canal and mental foramen associated to unilateral hemifacial microsomia, including hypoplasia of the facial musculature with a mild degree of microtia [9]. C. Herlin et al reported a very short course in the left IAC, opening onto the lateral surface of the mandibular angle. There was no other foramen on the lateral wall of the left mandibular body. No morphological abnormality of the face was noted on clinical examination [10].
Conclusions
Better understanding of the anatomic variation of the nerve may alter the planning of surgical procedures. Based on anatomical features and imaging findings, potential damage of the IAN during oral and dental operative treatment procedures in this region can be alleviated.
Financial Support
None.
| References | ▴Top |
- Rusu MC, Sandulescu M, Ciuluvica RC, Sendroiu VM, Didilescu AC. The extramandibular inferior alveolar nerve in cases with severely atrophic lower jaws. Surg Radiol Anat. 2012;34(3):277-279.
doi pubmed - Balaji SM, Krishnaswamy NR, Kumar SM, Rooban T. Inferior alveolar nerve canal position among South Indians: A cone beam computed tomographic pilot study. Ann Maxillofac Surg. 2012;2(1):51-55.
doi pubmed - Yeh AYE, Finn BP, Jones RHB, Goss AN. The variable position of the inferior alveolar nerve (IAN) in the mandibular ramus: a computed tomography (CT) study. Surg Radiol Anat. 2018;40(6):653-665.
doi pubmed - Worthington P. Injury to the inferior alveolar nerve during implant placement: a formula for protection of the patient and clinician. Int J Oral Maxillofac Implants. 2004;19(5):731-734.
pubmed - Mirbeigi S, Kazemipoor M, Khojastepour L. Evaluation of the course of the inferior alveolar canal: the first CBCT study in an Iranian population. Pol J Radiol. 2016;81:338-341.
doi pubmed - Khorshidi H, Raoofi S, Ghapanchi J, Shahidi S, Paknahad M. Cone beam computed tomographic analysis of the course and position of mandibular canal. J Maxillofac Oral Surg. 2017;16(3):306-311.
doi pubmed - Safaee A, Mirbeigi S, Ezoddini F, Khojastepour L, Navab-Azam A. Buccolingual course of the inferior alveolar canal in different mental foramen locations: A cone beam computed tomography study of an Iranian population. Int J Appl Basic Med Res. 2016;6(4):262-266.
doi pubmed - Ozturk A, Potluri A, Vieira AR. Position and course of the mandibular canal in skulls. Oral Surg Oral Med Oral Pathol Oral Radiol. 2012;113(4):453-458.
doi pubmed - Manikandhan R, Mathew PC, Naveenkumar J, Anantanarayanan P. A rare variation in the course of the inferior alveolar nerve. Int J Oral Maxillofac Surg. 2010;39(2):185-187.
doi pubmed - Herlin C, Yachouh J, Journet JL, Goudot P. Extramandibular position of the inferior alveolar nerve. Analysis and review of the literature. Surg Radiol Anat. 2013;35(9):811-815.
doi pubmed
This article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Medical Cases is published by Elmer Press Inc.