









| Journal of Medical Cases, ISSN 1923-4155 print, 1923-4163 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Med Cases and Elmer Press Inc |
| Journal website http://www.journalmc.org |
Case Report
Volume 3, Number 4, August 2012, pages 243-246
Choledochoduodenal Fistula Associated With Recurrent Peptic Ulcer
Takatsugu Yamamotoa, b, Koichiro Abea, Hajime Anjikia, Taro Ishiia, Yasushi Kuyamaa
aDepartment of Internal Medicine, Teikyo University School of Medicine, Tokyo, Japan
bCorresponding author: Takatsugu Yamamoto, Department of Internal Medicine, Teikyo University School of Medicine, 2-11-1 Kaga, Itabashi-ku, 173-8605, Tokyo, Japan
Manuscript accepted for publication February 23, 2012
Short title: Choledochoduodenal Fistula
doi: https://doi.org/10.4021/jmc595w
| Abstract | ▴Top |
A male 33 years of age who had a history of recurrent duodenal ulcer was admitted to our hospital because of frequent vomiting and weight loss. The blood tests showed hypokalemia and acute renal dysfunction due to dehydration. Abdominal CT revealed dilatation of the stomach with pneumobilia of the intrahepatic bile duce, and endoscopy showed duodenal ulcer with stricture of the duodenal bulb. The diagnosis of choledochoduodenal fistula due to duodenal ulcer was made, so he underwent surgical operation because the obstruction was severe. Both choledochobiliary fistula and duodenal stricture are relatively rare complications of duodenal ulcer. Here we report on a case accompanied by the both complications, requiring surgical operation.
Keywords: Duodenal ulcer; Fistula; Biliary tract
| Introduction | ▴Top |
Peptic ulcer is common condition in Japan because of high prevalence of Helicobacter pylori infection. However, severe complications such as entero-biliary fistula are relatively rare in recent years due to development of strong acid suppressants. Here we report on a case with recurrent duodenal ulcer accompanied by choledochobiliary fistula and duodenal stricture which require surgical operation.
| Case Report | ▴Top |
A 33-year-old male visited to Teikyo University Hospital (Tokyo, Japan) because of recurrent vomiting and marked weight loss (20 kg/year). He had a 15-year history of recurrent duodenal ulcer (Fig.1). Last year, he was recommended by a physician to have eradication therapy against Helicobacter pylori, but, he did not. On admission, the laboratory data showed acute renal dysfunction due to dehydration and hypokalemia (Table 1). Abdominal computed tomography revealed dilatation of the stomach and the air in the intrahepatic biliary duct (Fig. 2). Esophagogastroduodenoscopy showed marked deformity with severe stricture of the duodenal bulb (Fig. 3). Although the presence of hole could not be confirmed directly, gastroduodenography showed contrast medium entered into the biliary tract, indicating duodeno-biliary fistula (Fig. 4). He could not take meal enough due to duodenal stricture, so partial gastroduodenectomy was performed. After the operation, he had been able to eat meals and was discharged without serious complication.
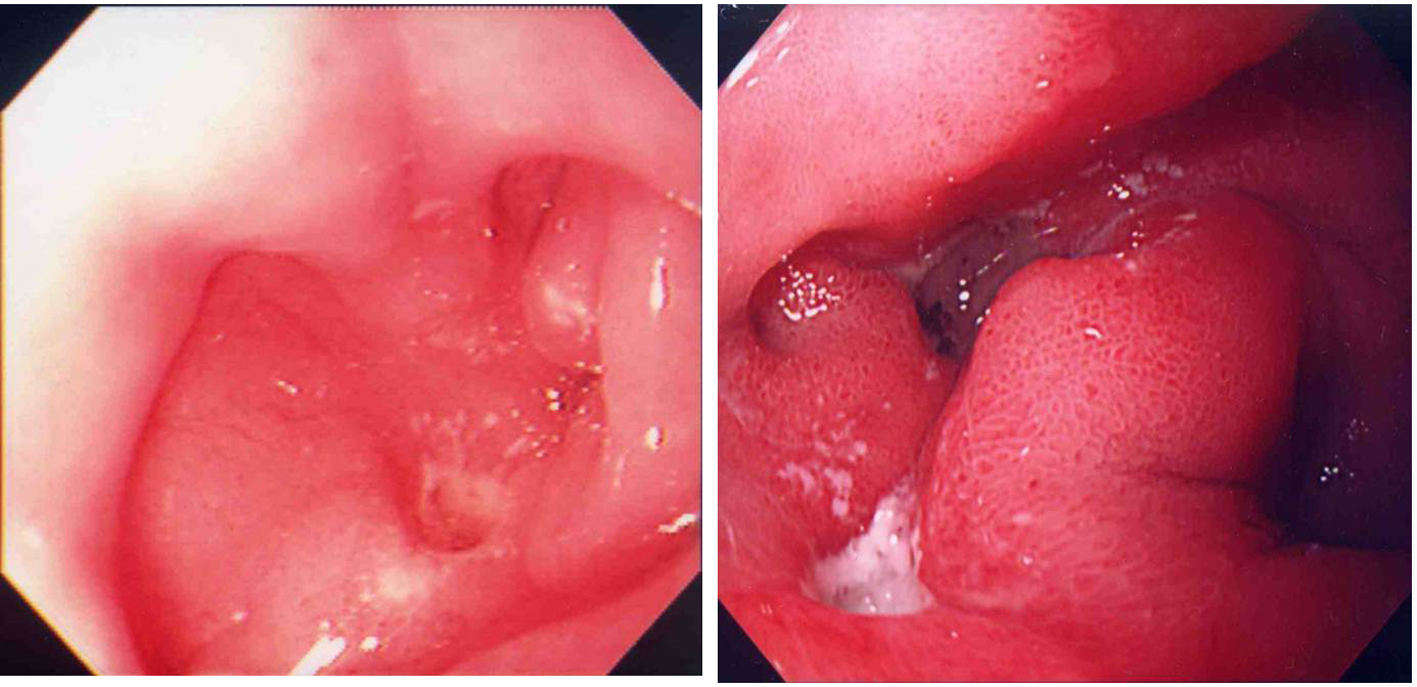 Click for large image | Figure 1. Past endoscopic findings; 19 years old (left) and 32 years old (right). |
 Click to view | Table 1. Laboratory Data |
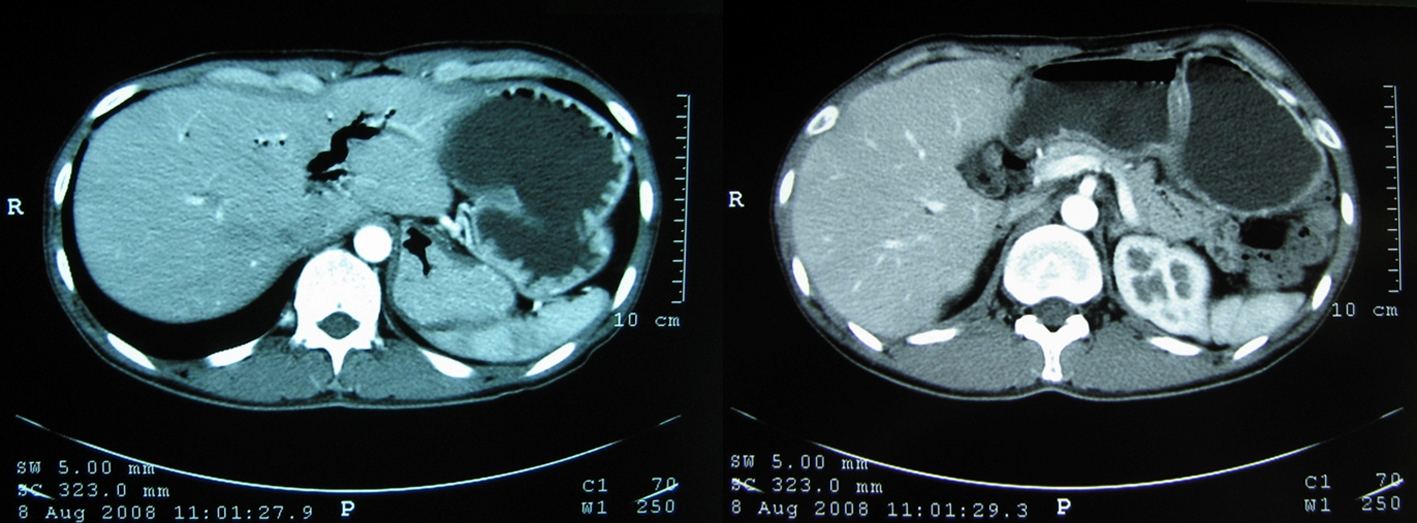 Click for large image | Figure 2. Abdominal computed tomography. Peumobilia in the intrahepatic bile duct (left) and dilatation of the stomach (right) was found. |
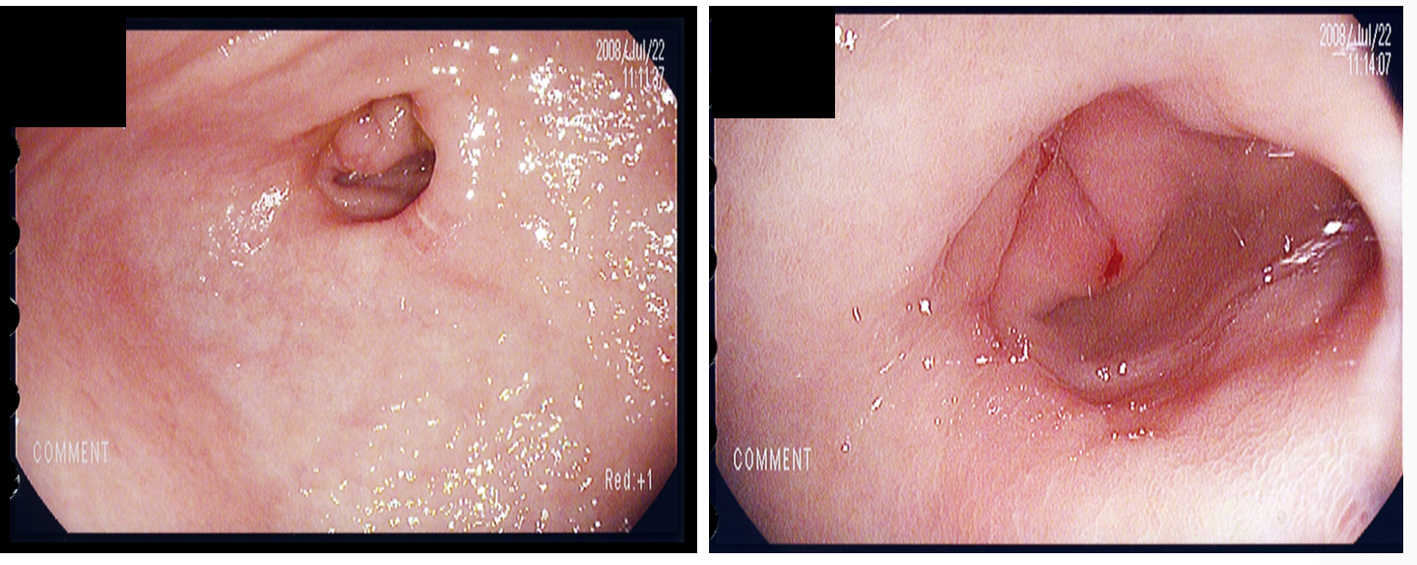 Click for large image | Figure 3. Upper gastrointestinal endoscopy. Duodenal ulcer and stricture was seen. |
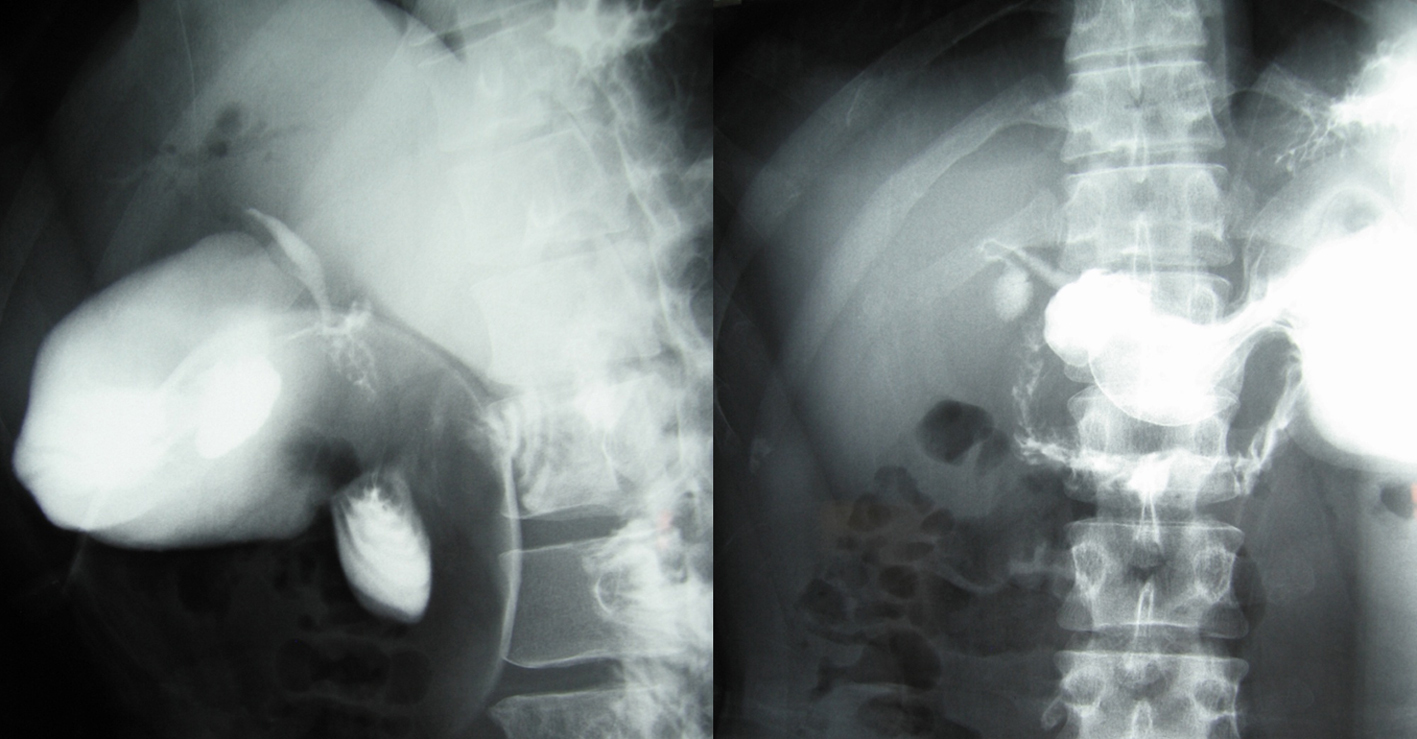 Click for large image | Figure 4. Upper gastoduodenography. This revealed the existence of choledochoduodenal fistula. |
| Discussion | ▴Top |
Choledochoduodenal fistula is well-known but a relatively rare complication of duodenal ulcer in recent years, because the development of antiacid drugs makes us control the disease easier than before. The most major cause for duodeno-biliary fistula is inflammation of the bile duct due to gallstones, and the minors include duodenal ulcer, pancreatic neoplasm, and inflammation of neighbor organs [1-2]. Yamashita et al. reported that 33 of 1929 cases (1.9%) with biliary diseases showed duodeno-biliary fistula [3]. On the other hand, duodenal ulcer causes fistula to the other organs such as the biliary tract, pancreas, ureter, portal vein, aorta, pleura and skin [3-8]. Of these, biliary fistula seems more often than others [9]. Stricture is also uncommon condition of duodenal ulcer. In the present case, both the complications occurred as a result of recurrence of the disease. Additionally, the stricture of the duodenum got him unable to take food and water, developing weight loss and acute renal dysfunction due to dehydration.
Possible treatments of both complications include surgical therapy, endoscopy, and conservative treatment [10]. Endoscopic therapy such as endoscopic closure and dilatation, may be an alternative method for surgery. In our case, however, both fistula and stricture coexisted, and endoscopic closure was not available because the location of the fistula could not be confirmed precisely. Additionally, since the stricture was very severe, we could not try endoscopic dilatation. Then we did not choose endoscopic or conservative treatment, but did surgical operation.
Here we reported on a rare case of duodenal ulcer accompanied by duodeno-biliary fistula and duodenal stricture. Since duodenal ulcer is common condition, we need to remind those complications and treatment against them.
| References | ▴Top |
- Sharma K, Kibria R, Ali S, Rao P. Primary aortoenteric fistula caused by an infected abdominal aortic aneurysm with Mycobacterium avium complex in an HIV patient. Acta Gastroenterol Belg. 2010;73(2):280-282.
pubmed - Miyamoto S, Furuse J, Maru Y, Tajiri H, Muto M, Yoshino M. Duodenal tuberculosis with a choledocho-duodenal fistula. J Gastroenterol Hepatol. 2001;16(2):235-238.
pubmed doi - Yamashita H, Chijiiwa K, Ogawa Y, Kuroki S, Tanaka M. The internal biliary fistula—reappraisal of incidence, type, diagnosis and management of 33 consecutive cases. HPB Surg. 1997;10(3):143-147.
pubmed doi - Kinoshita H, Takifuji K, Nakatani Y, Tani M, Uchiyama K, Yamaue H. Duodenoportal fistula caused by peptic ulcer after extended right hepatectomy for hilar cholangiocarcinoma. World J Surg Oncol. 2006;4:84.
pubmed - Nwose PE, Nwofor AM, Ogbuokiri UC. Duodeno-pleural fistula: a rare complication of peptic ulcer perforation. Niger J Clin Pract. 2006;9(1):84-86.
pubmed - Sotiropoulos GC, Oldhafer KJ, Fruhauf NR, Treichel U, Clauer UA, Brokalaki EI, Broelsch CE. Jejunoduodenal fistula due to penetrating peptic ulcer after Roux-en-Y hepaticojejunostomy. Endoscopy. 2003;35(6):549.
pubmed doi - Tan SM, Teh CH, Tan PK. Duodeno-ureteric fistula secondary to chronic duodenal ulceration. Ann Acad Med Singapore. 1997;26(6):850-851.
pubmed - Shiwani MH. Cholecystoduodenal fistula secondary to penetrating duodenal ulcer: a case of conservative management. J Coll Physicians Surg Pak. 2006;16(1):83-84.
pubmed - Jaballah S, Sabri Y, Karim S. Choledochoduodenal fistula due to duodenal peptic ulcer. Dig Dis Sci. 2001;46(11):2475-2479.
pubmed doi - Yamamoto T, Allan RN, Keighley MR. An audit of gastroduodenal Crohn disease: clinicopathologic features and management. Scand J Gastroenterol. 1999;34(10):1019-1024.
pubmed doi
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Medical Cases is published by Elmer Press Inc.