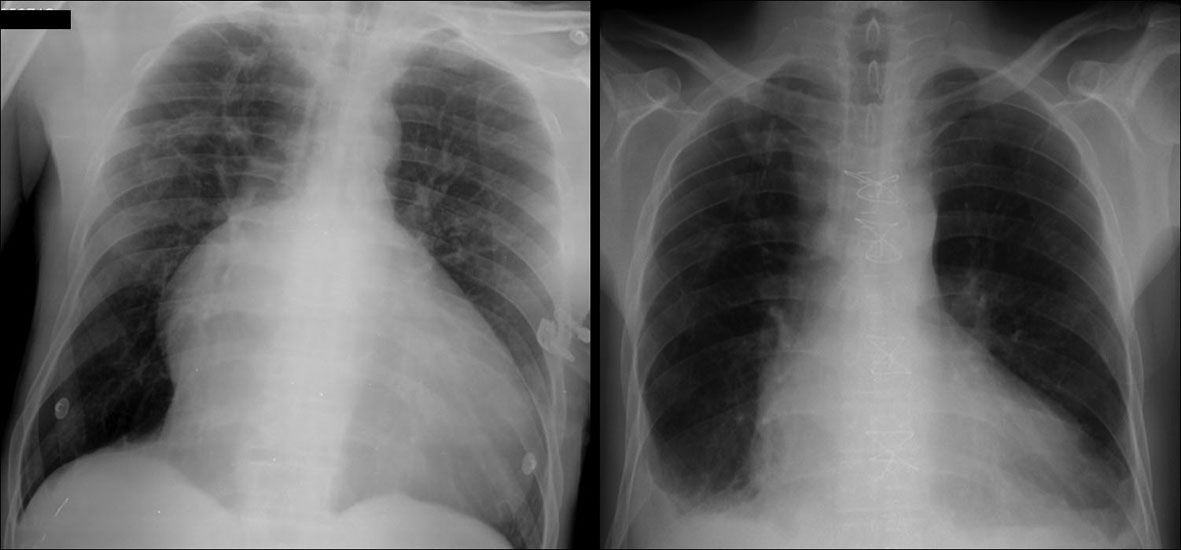
Figure 1. Chest radiograph. Left figure: chest X-ray on Emergency Room’s admission revealed significant cardiomegaly, prominent right atrium and straight left heart border. Right figure: imaging at postoperative image showed close-to-normal anatomical configuration of the heart as a result of major heart plasty.
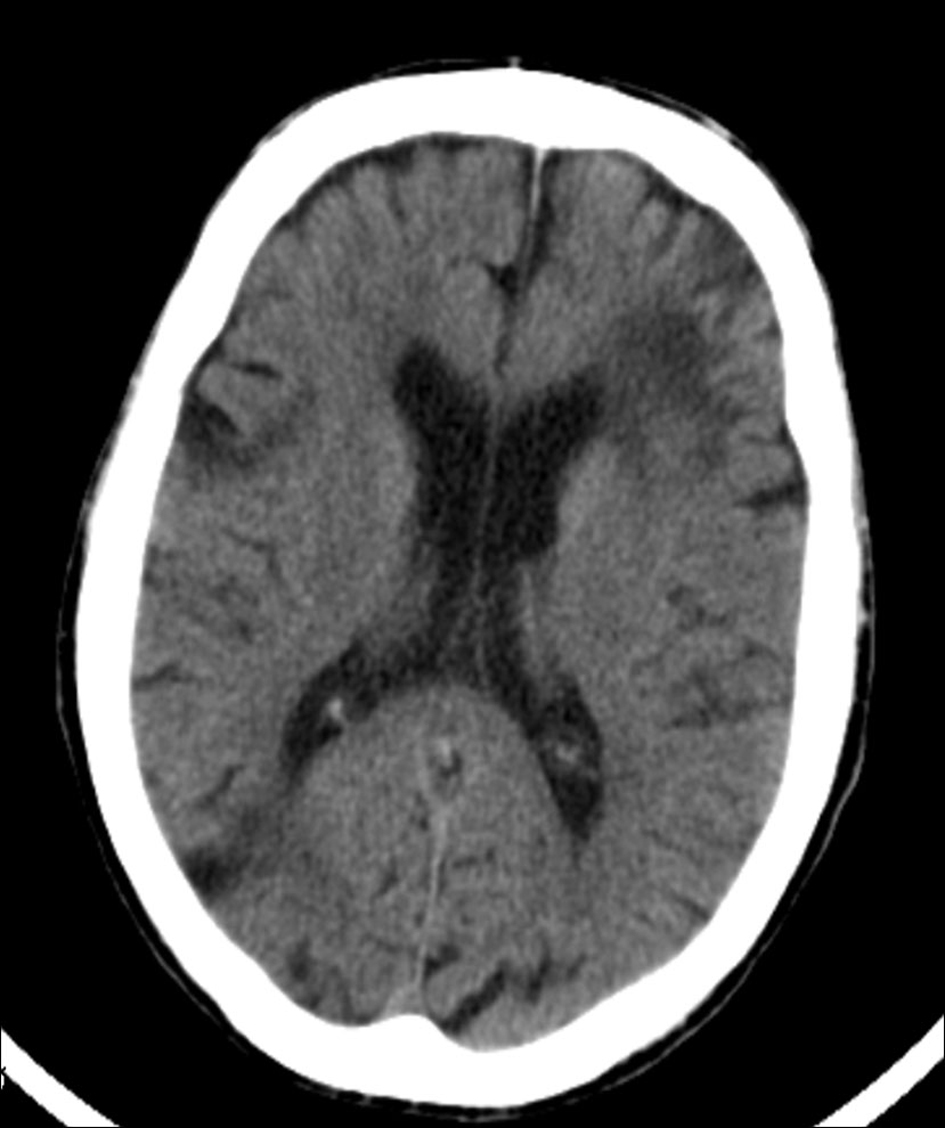
Figure 2. Head computed tomography scan revealed an extensive left frontal corticosubcortical ischemic lesion, and other significant ischemic foci at the head of the right caudate nucleus. Sequelae of focal ischemic lesions were additionally seen scattered through the brain and cerebellum.
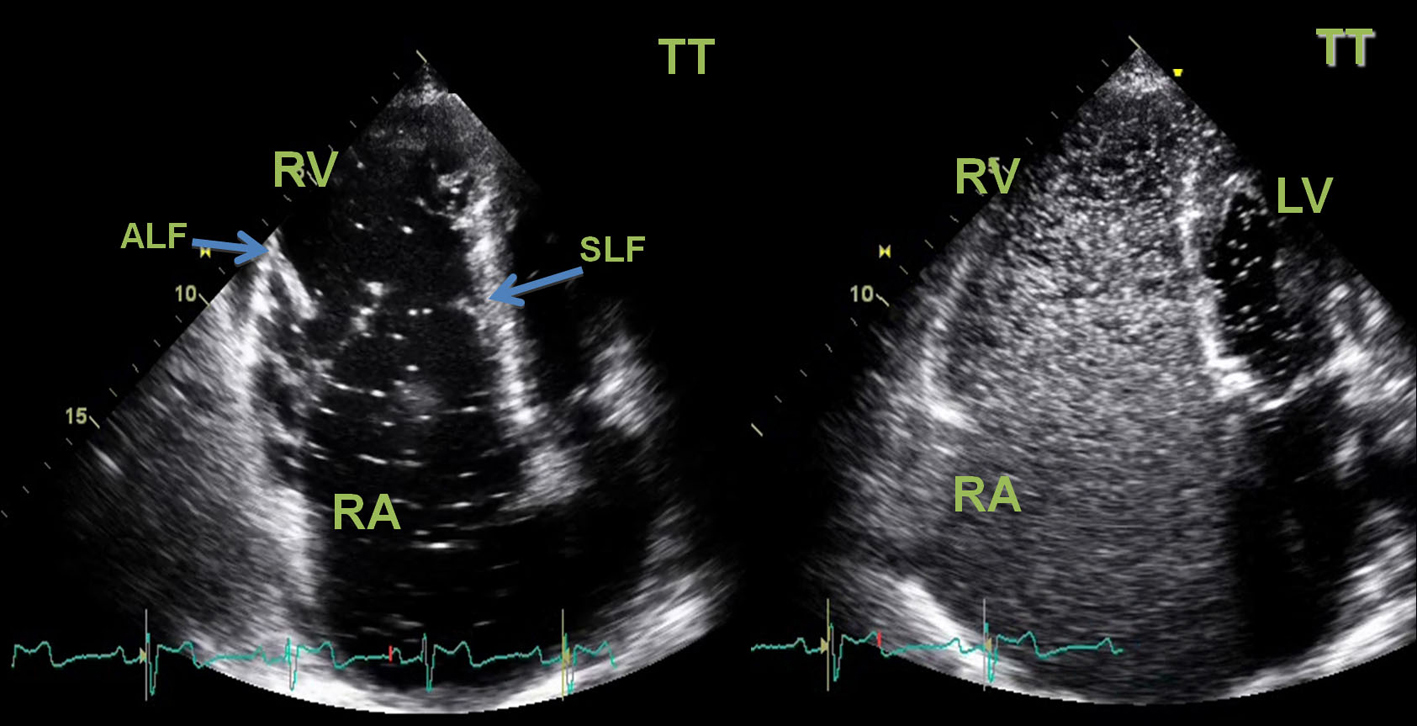
Figure 3. Two-dimensional transthoracic (TT) echocardiogram. Left image: apical chamber view showed a severe right atrial aneurismatic dilatation, an asymmetric tricuspid valve with a “sail-like” structure, tethering of the septal leaflet with distal implantation at 8.1 cm/m2(atrialized right ventricle). The tricuspid valve leaflets were dysplastic and major defect of central coaptation was observed resulting in severe tricuspid failure. Right ventricle systolic function was severely compromised. Diastolic flattening of interventricular septum and paradoxical septal motion was seen in favour of right ventricular overload. Left chambers had normal dimensions and left ventricle systolic function was preserved. No vegetations or thrombus were seen. Right Image: passage of agitated saline contrast from right to left chambers through an interatrial communication was documented (white spots on LV area) in favor of the presence of a right-to-left shunt. RA: right atrium; RV: right ventricle; LA: left atrium; LV: left ventricle; SLF: septal leaflet; ALF: anterior leaflet.