Figures
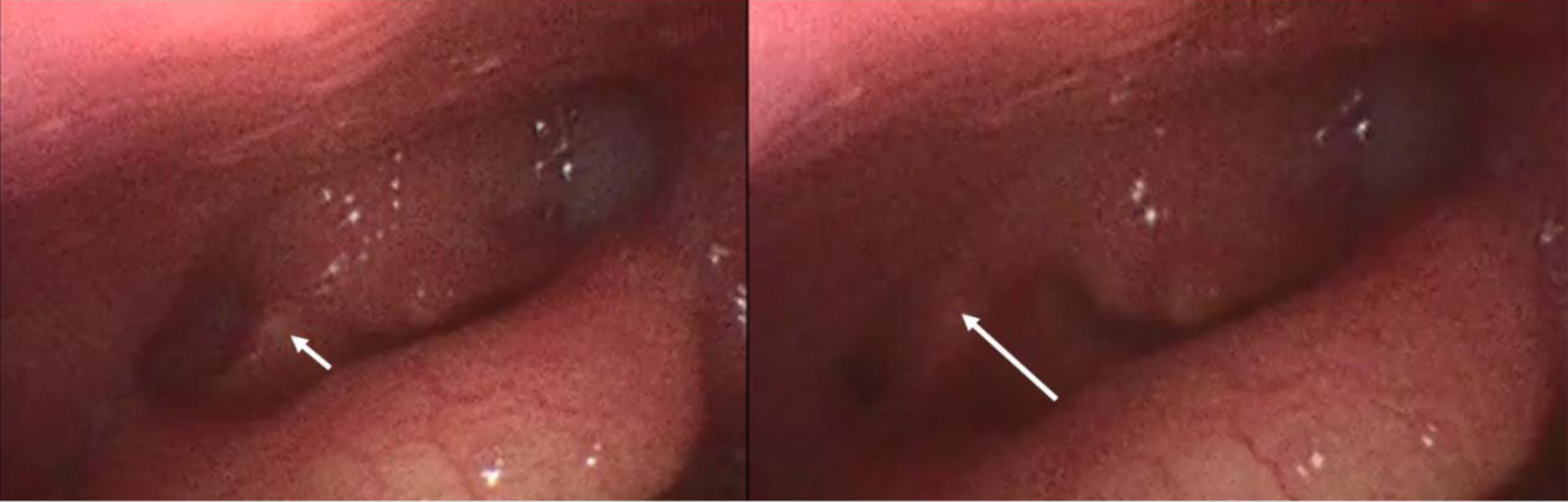
Figure 1. Complete left hemilarynx paralysis. During phonation, the correct motility of the right arytenoid cartilage is visible (white arrow).
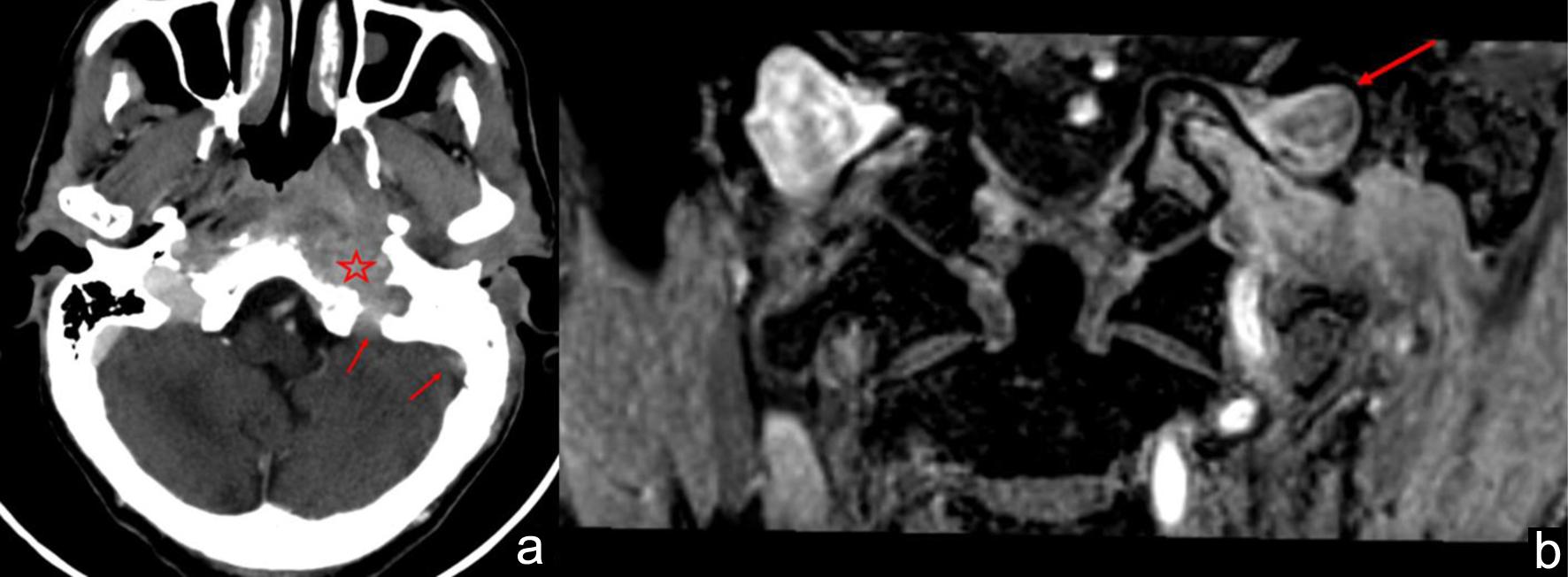
Figure 2. (a) Computed tomography (CT) scan after the administration of contrast medium shows thrombosis of the sigmoid sinus and jugular bulb (red arrows), which is inseparable from the pathological tissue (red star). (b) Magnetic resonance imaging (MRI) coronal T1w image after gadolinium administration. Thrombosis of jugular bulb (red arrow).
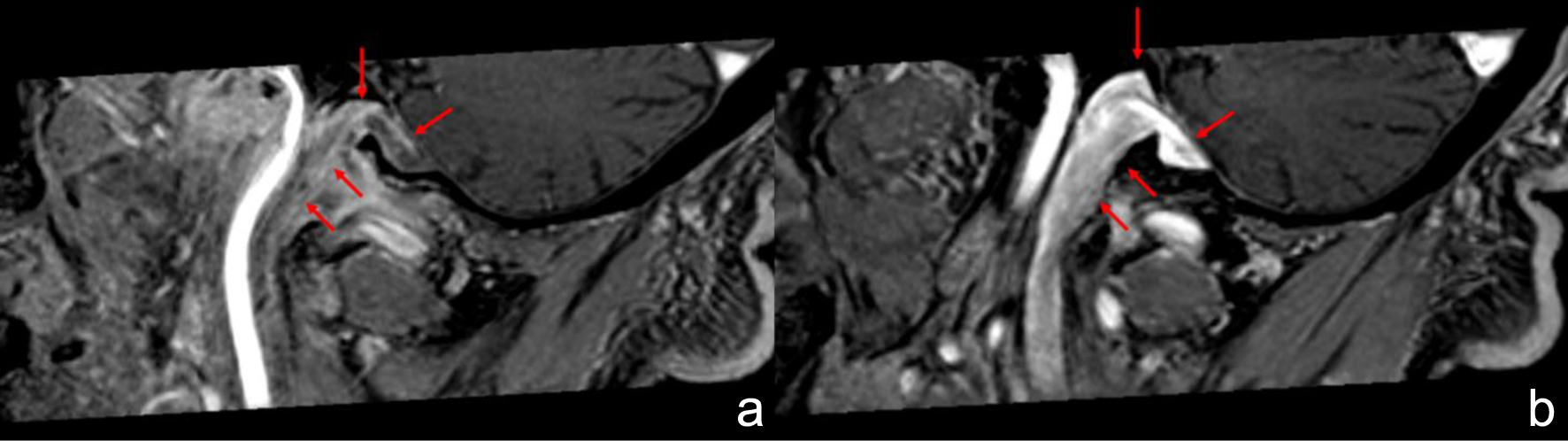
Figure 3. Magnetic resonance imaging (MRI) sagittal T1w image after gadolinium administration. (a) Thrombosis of sigmoid sinus and internal jugular vein (red arrows). (b) Right normal side, demonstrating normal appearance of sigmoid sinus and internal jugular vein (red arrows).
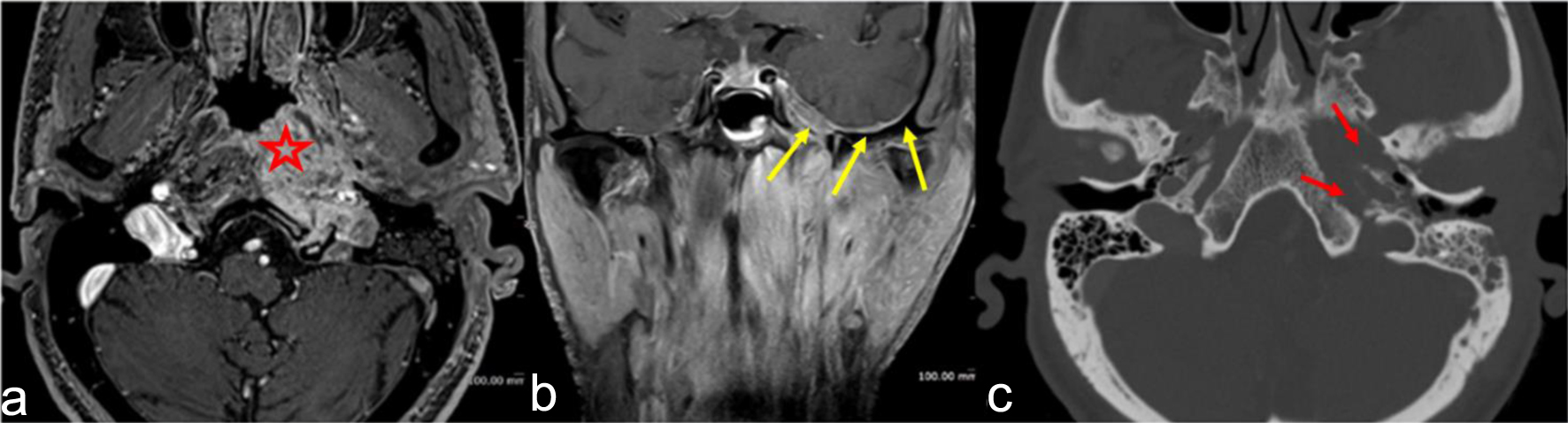
Figure 4. Magnetic resonance images in contrast-enhanced sequences, axial (a) and coronal (b). Axial cut in computed tomography (CT) (c). Infiltrative soft tissue mass in the deep spaces of the suprahyoid neck deforms the nasopharynx (red star); ipsilateral infiltration and erosion are noted on the clivus and petrous apex (red arrows). Pathological tissue extends to the oval foramen; dural thickening and enhancement on the middle cranial fossa floor and Meckel’s fossa are appreciated (yellow arrows).

Figure 5. Left abducens nerve palsy.