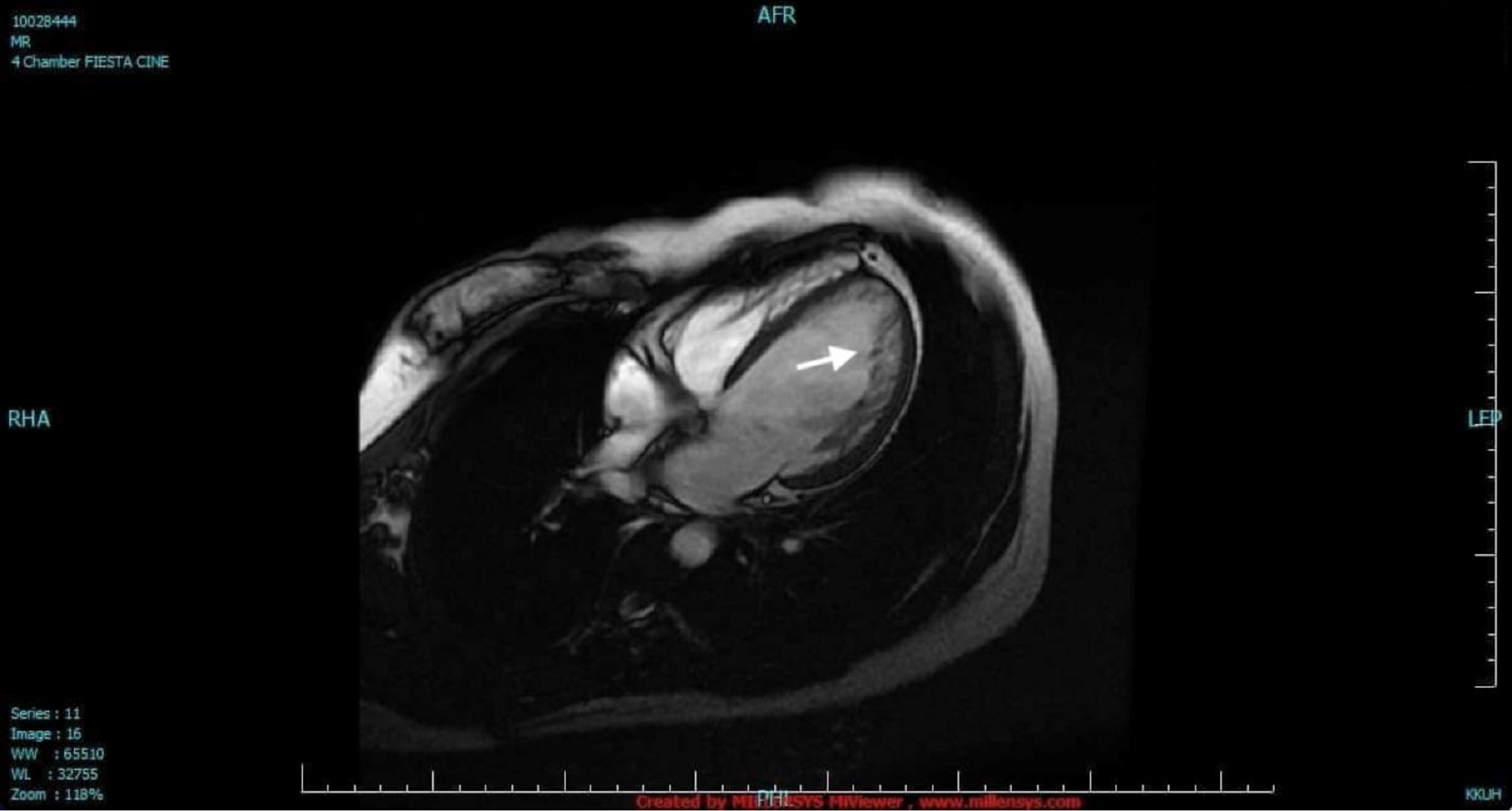
Figure 1. Cardiac magnetic resonance imaging. The LV was dilated with two distinct myocardial layers: a compact layer and a noncompact layer with prominent trabeculations and deep intertrabecular recesses in the lateral wall from base to apex (arrow). The LV systolic function was moderately to severely depressed. LV: left ventricle.