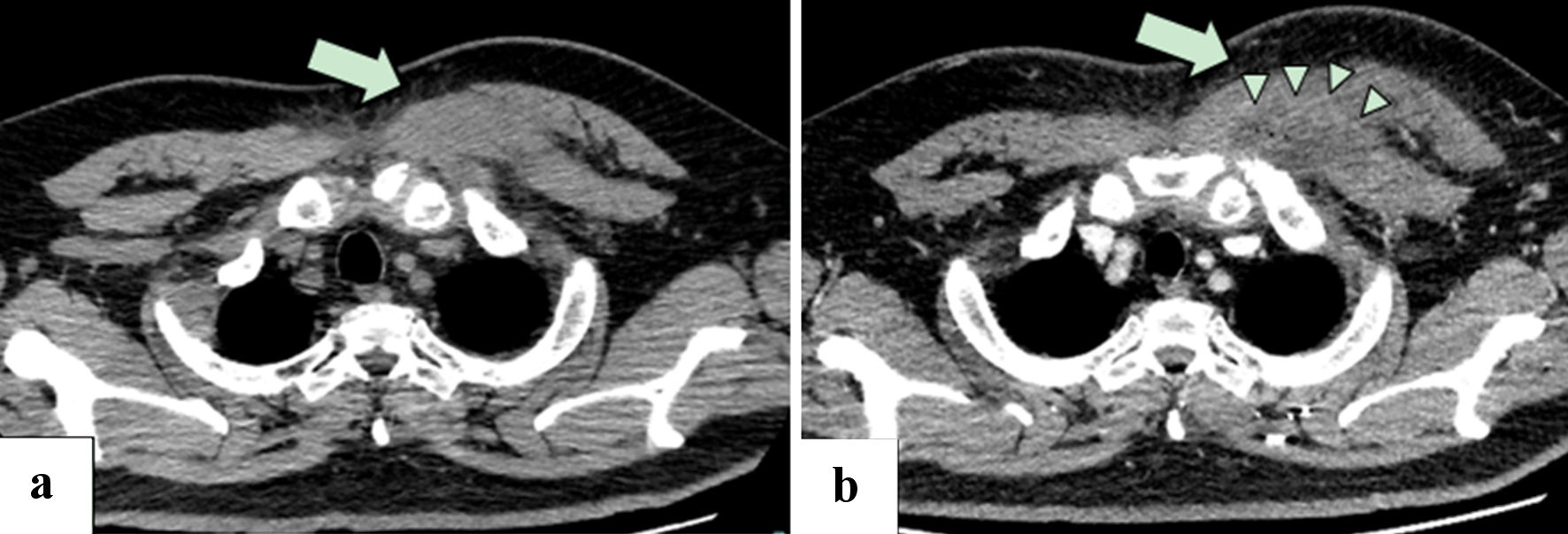
Figure 1. (a) Plain CT of the chest 1 day before admission showed swelling of the left major pectoralis muscle, with subcutaneous fat stranding (arrow). (b) Contrast-enhanced CT of the chest on day 3 of hospitalization showed a poor contrast enhancement area in the swelling of the major pectoralis muscle with ring-enhancement (arrow) and minute gas production (arrow heads), suggesting abscess formation. Left pleural effusion was revealed. CT: computed tomography.
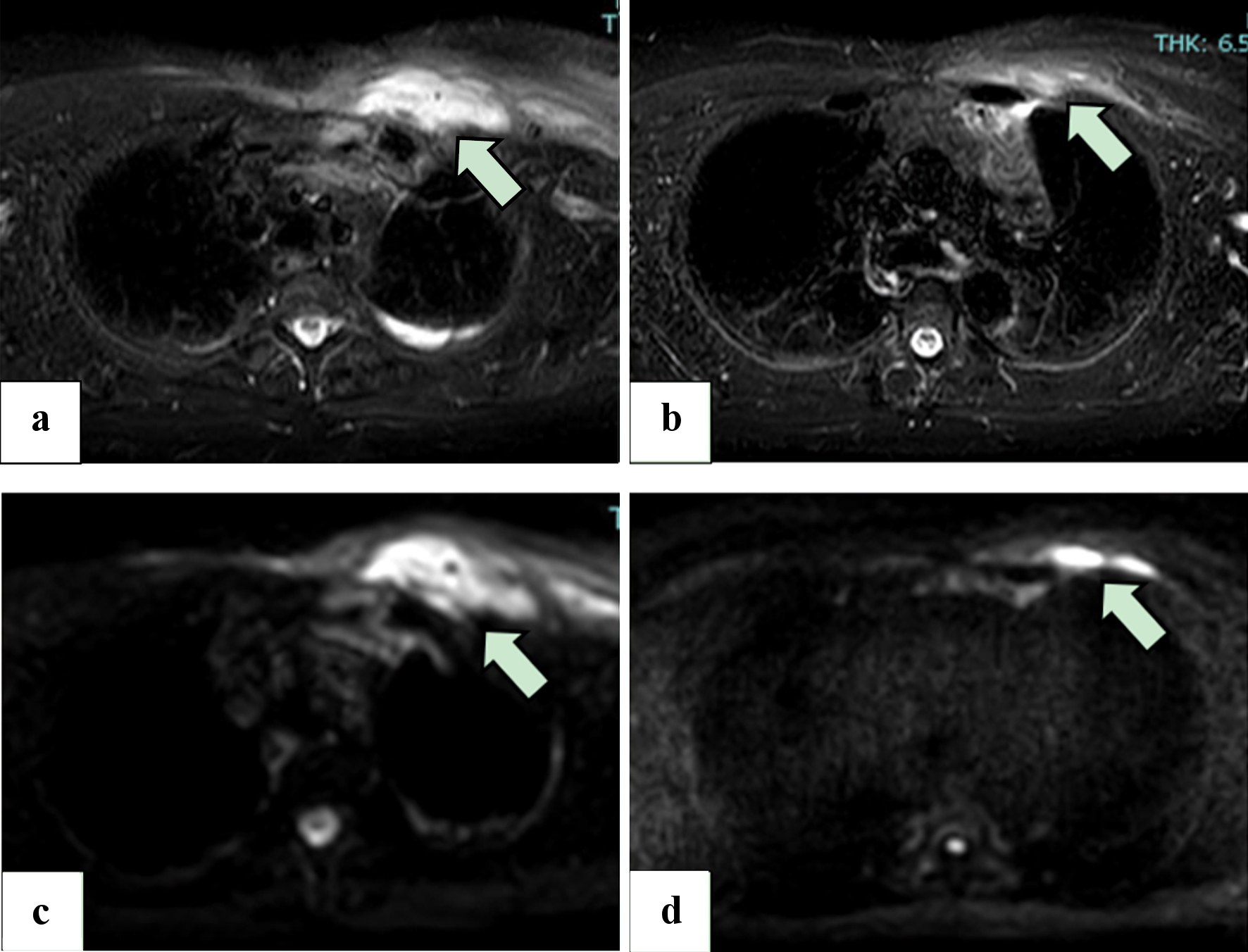
Figure 2. (a, b) STIR images from the MRI scan on day 10 of hospitalization (a) and 11 days after hospital discharge (b), without intravenous administration of gadolinium. Areas of high signal (arrow) reduction indicate that the swelling of the left pectoralis major has improved. (c, d) DWI MRI scans of the chest on day 10 of hospitalization (c) and 11 days after hospital discharge (d), without intravenous administration of gadolinium. The volume of the abscesses in the pectoralis major muscle (arrow) has been reduced. MRI: magnetic resonance imaging; STIR: short tau inversion recovery; DWI: diffusion-weighted imaging.