Figures
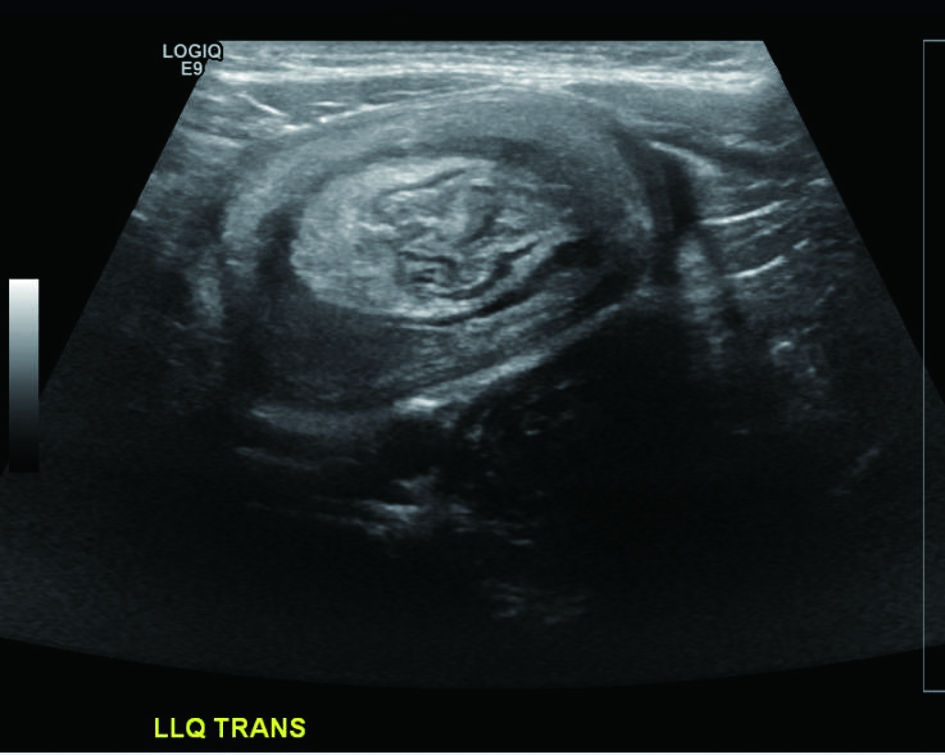
Figure 1. Transverse ultrasound image of the left lower quadrant demonstrates a mass with a “target” sign.

Figure 2. Air enema demonstrates a filling defect in the descending colon surrounded by a crescent of air representing the intussusceptum. Real time images demonstrated retrograde movement of the filling defect as the intussusception was reduced.
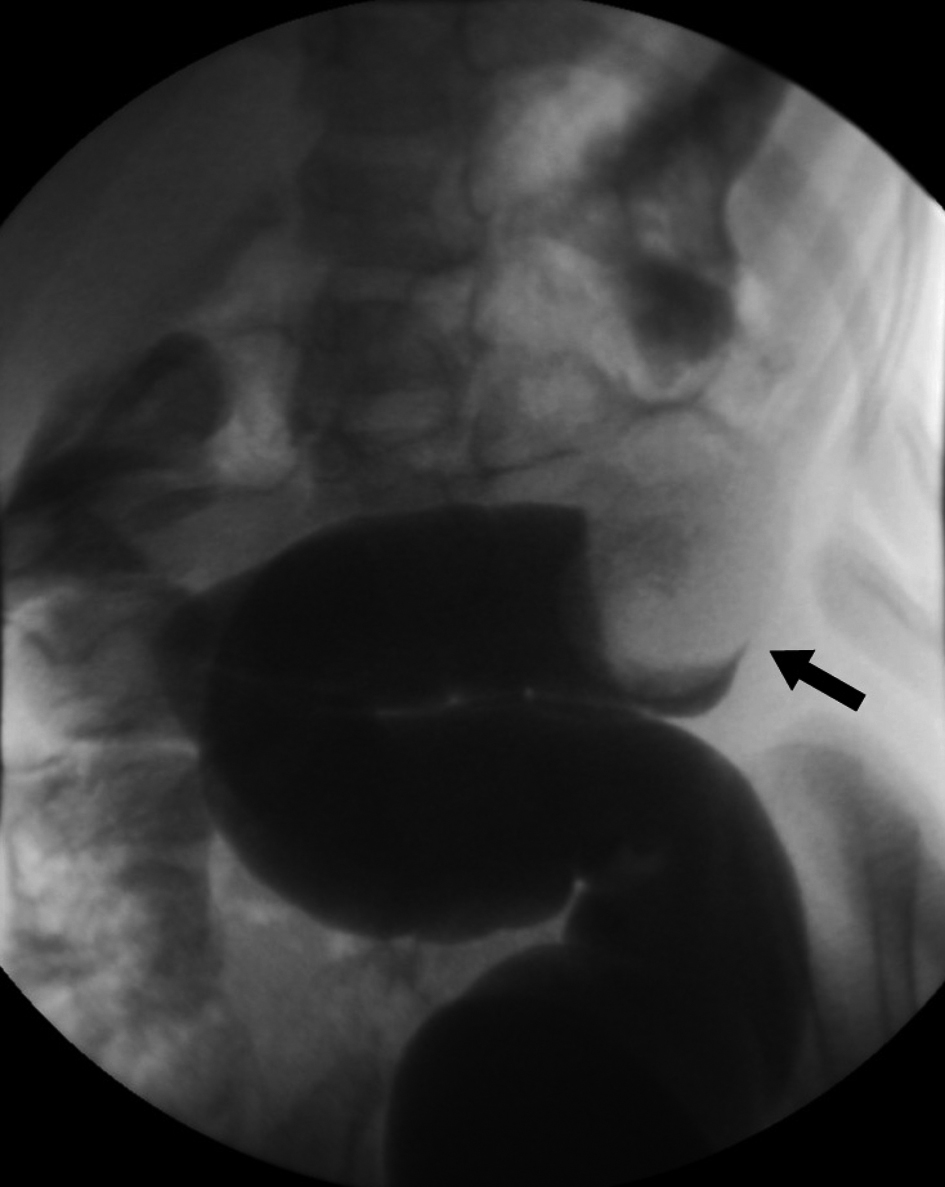
Figure 3. Single contract enema again shows a filling defect in the colon, representing the intussusceptum.
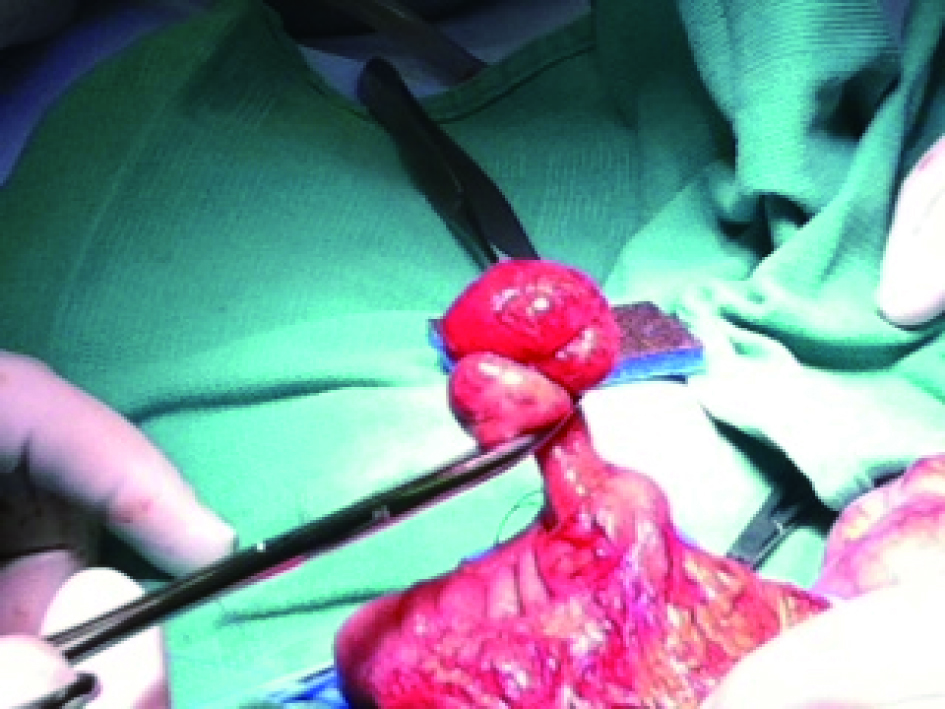
Figure 4. Pedunculated juvenile polyp is isolated from the mesenteric side of the transverse colon mucosa for surgical excision.
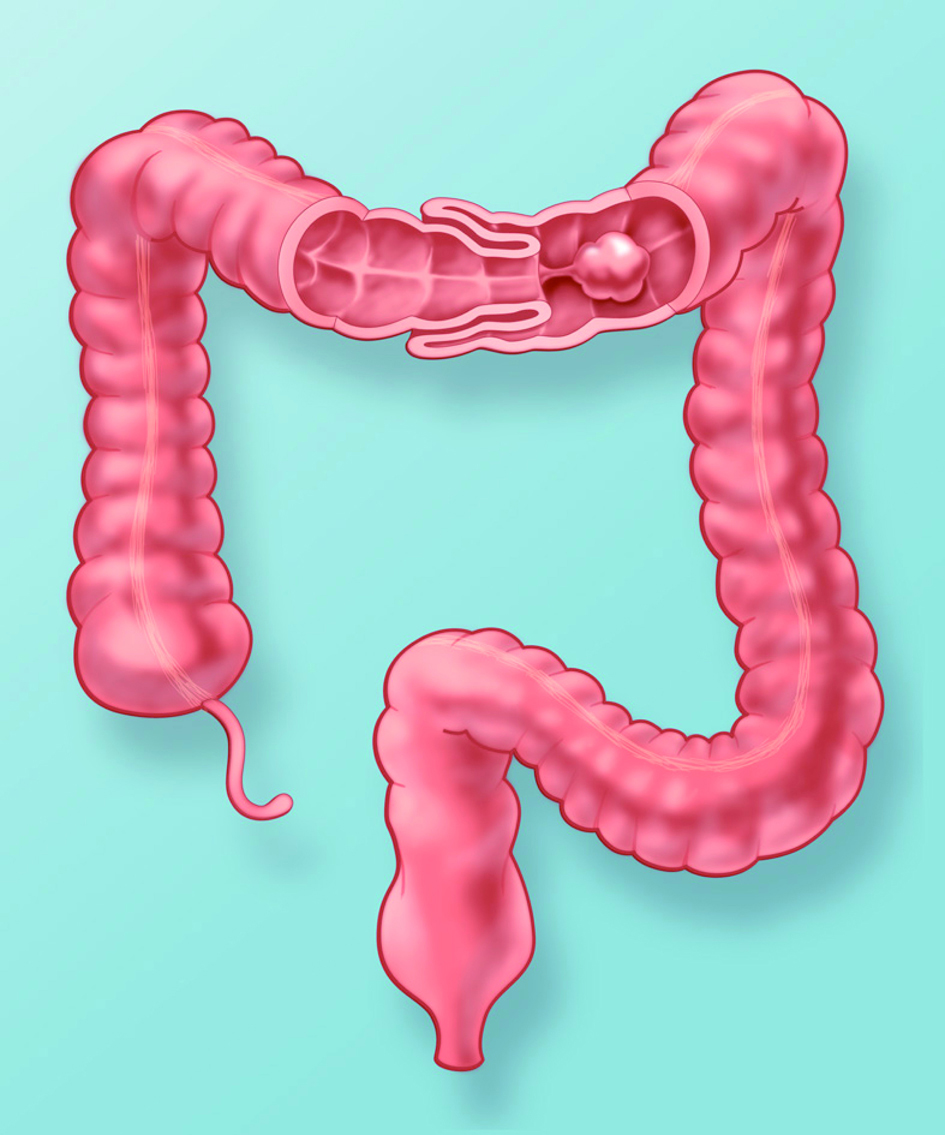
Figure 5. Artist’s rendering of the colon with coronal window through the transverse colon demonstrates intussusception secondary to a pedunculated polyp. Peristalsis pulls the large polyp distally, dragging the attached bowel wall into the intussuscipient.
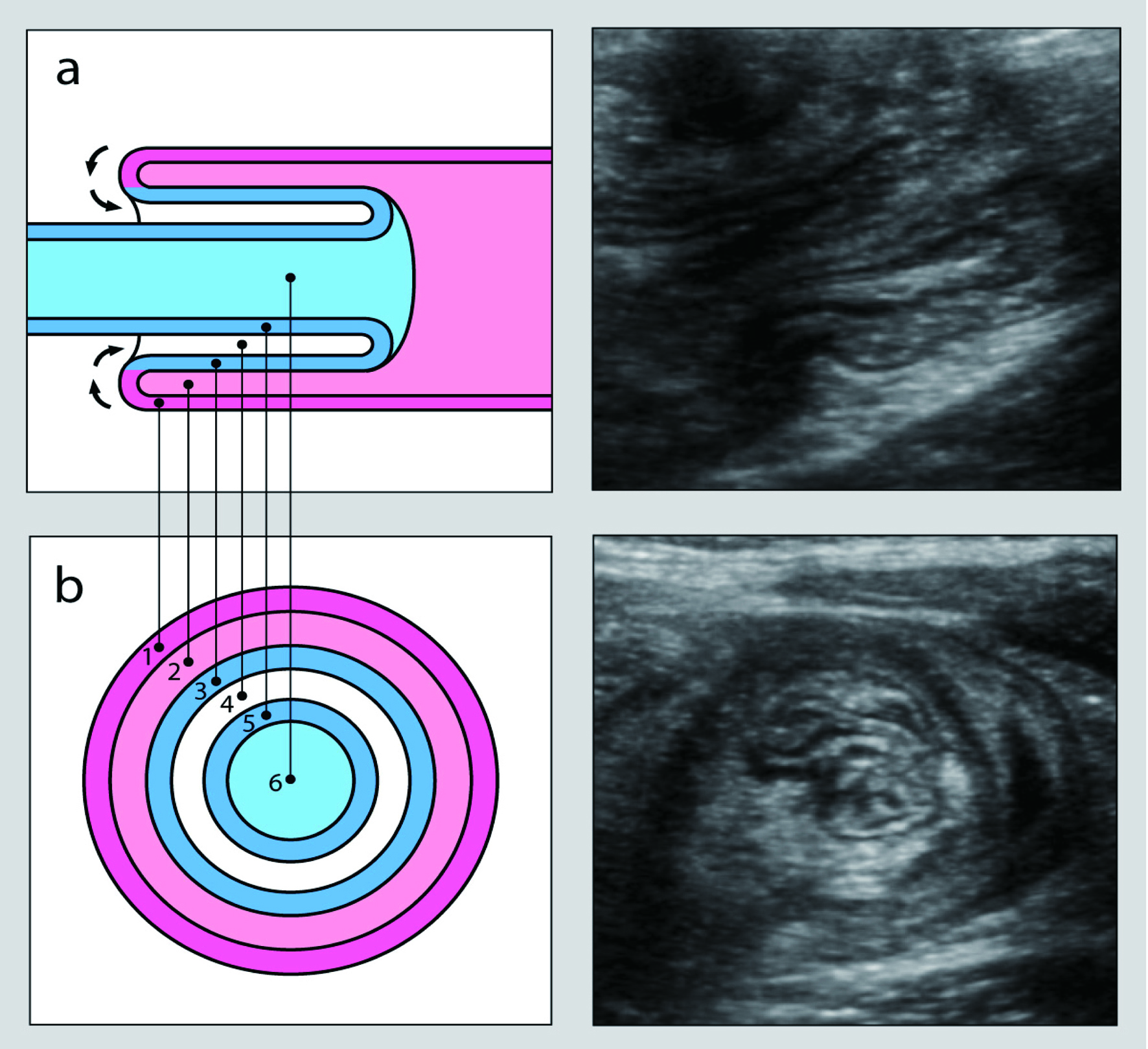
Figure 6. Longitudinal (a) and transverse (b) cross-sectional views of an intussusception. Images on the left graphically represent the intussusception complex while corresponding ultrasound images are depicted on the right. The outer layers represent the intussuscepient while the inner layers represent the intussusceptum. The bowel wall (1) and lumen (2) of the intussuscepient make up the outer rings. The inner rings are comprised of the bowel wall (3 and 5) and lumen (6) of the intussusceptum surrounded by mesenteric fat (4). In vivo, the lumen is collapsed and the echogenic rings on ultrasound represent interfaces between the mucosa, submucosa, muscularis, and serosa.