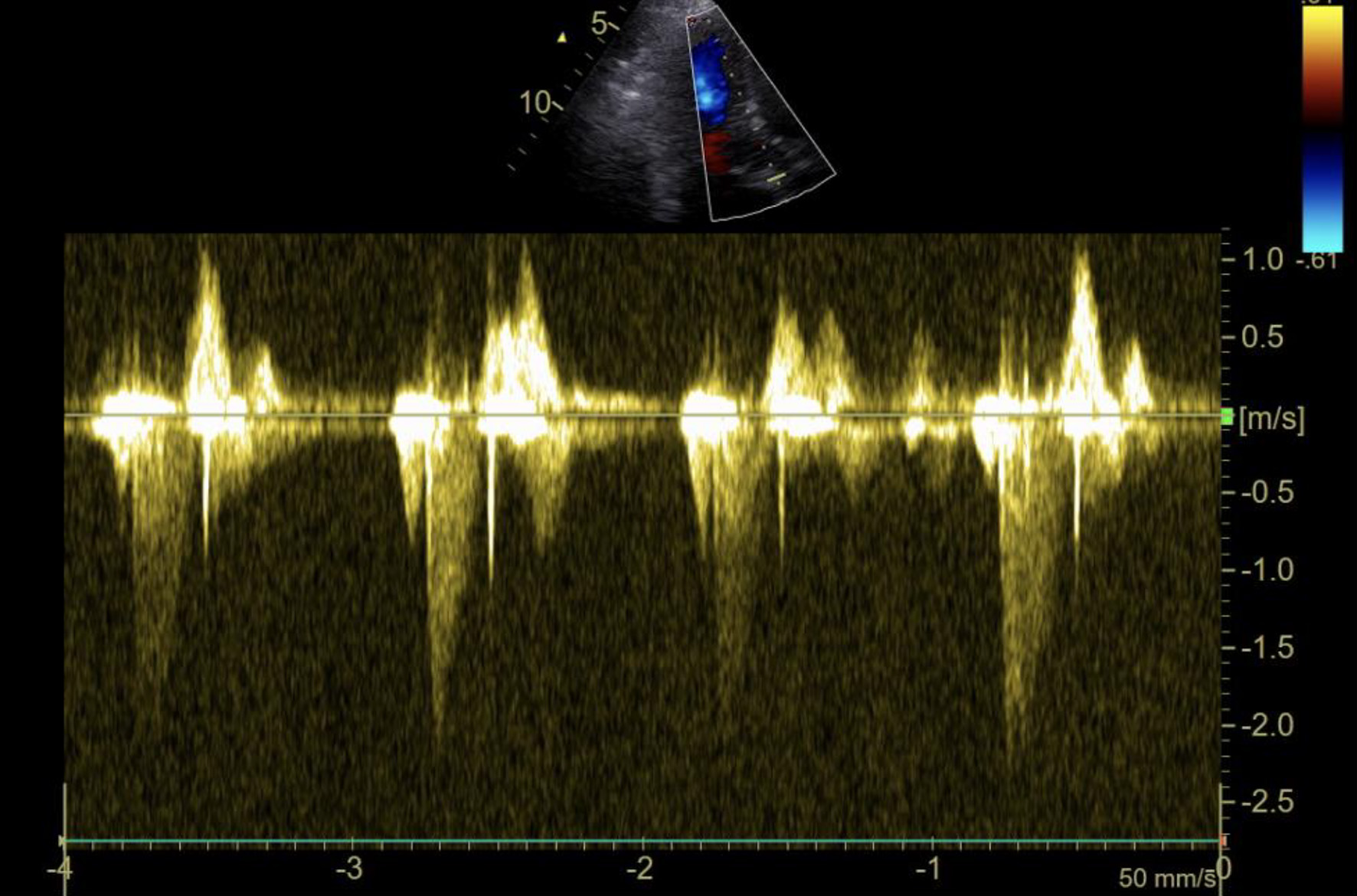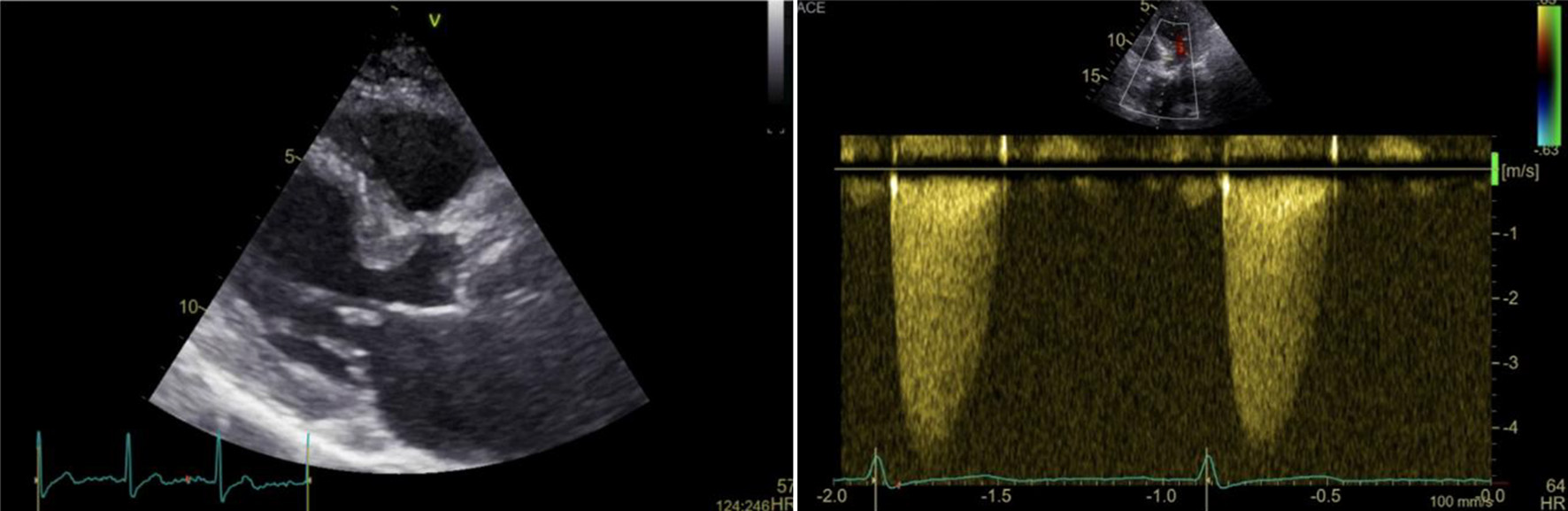
Figure 1. Transthoracic echocardiography of the bioprosthetic aortic valve: 2D picture showing thickened left ventricular septum and severely calcified aortic cusps (left); continuous doppler through the bioprosthetic aortic valve showing severe stenosis (maximal velocity 4.3 m/s, mean gradient 43 mm Hg) (right).
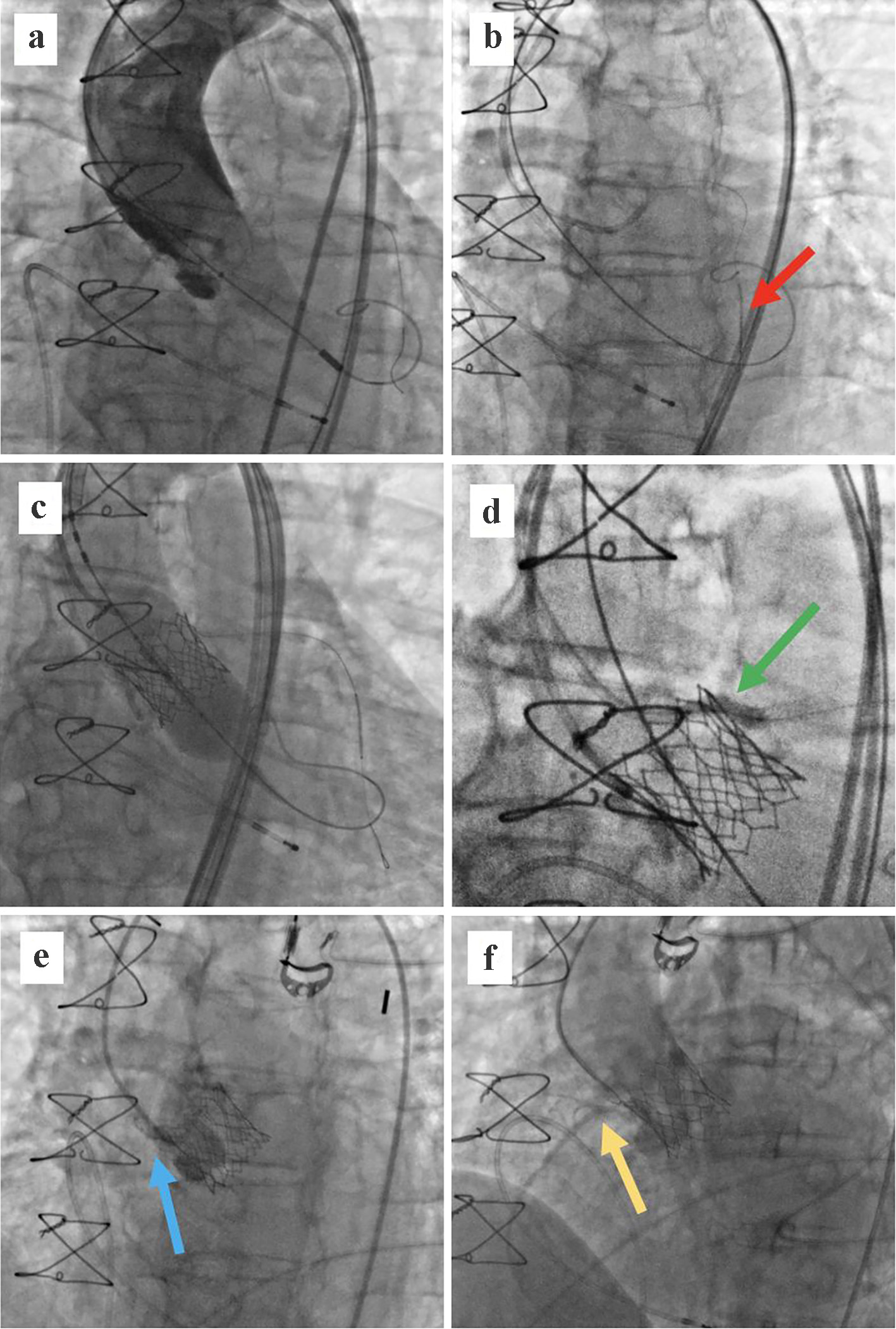
Figure 3. (a) Balloon aortic valvuloplasty with a 22 × 40 mm balloon and a BMW wire placed in the distal LAD. Flow is present in both coronary arteries. (b) Drug-eluted stent placed in the middle segment of the LAD (red arrow). (c) Implantation of a 26-mm balloon-expandable Sapien 3 valve in the annular position. (d) Left main stenting up to the ascending aorta using the “chimney technique”; post-dilatation balloon (green arrow). (e) Aortography showing an occlusion of the RCA (blue arrow). (f) Flow restoration in the RCA after administration of unfractionated heparin and eptifibatide (yellow arrow). LAD: left anterior descending; RCA: right coronary artery.