Figures
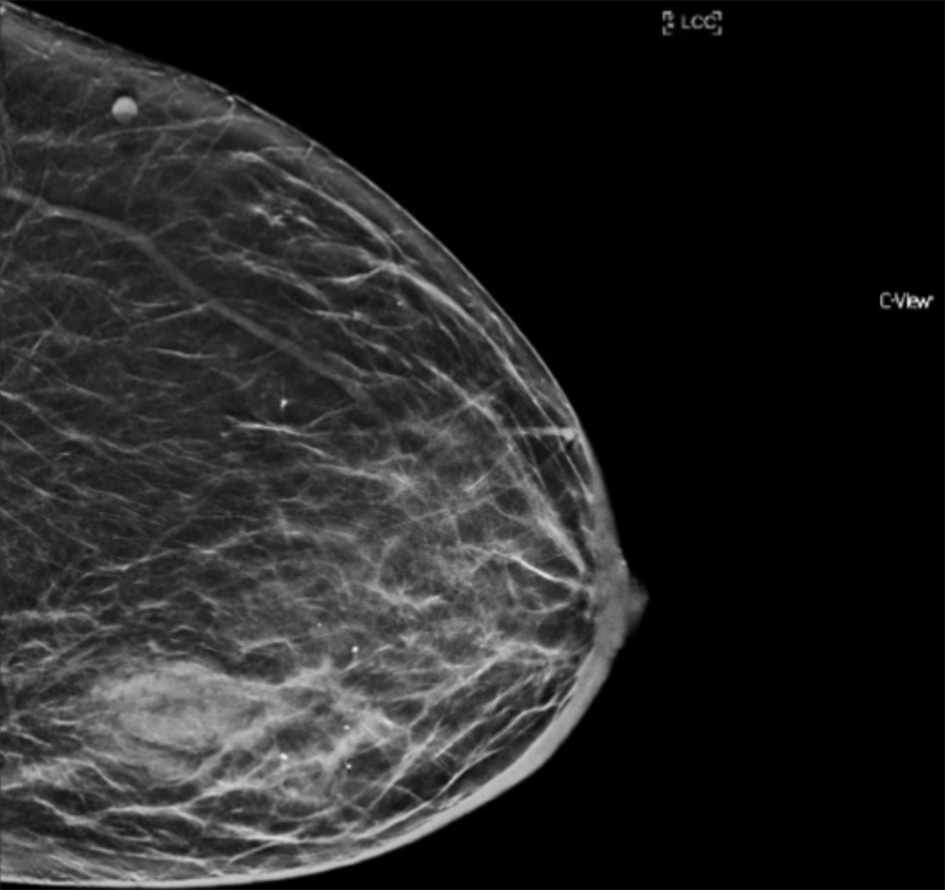
Figure 1. Mammogram of left breast (cranio-caudal view) with poorly circumscribed mass, measuring 40 × 24 mm, in the lateral aspect of breast at the level of the nipple. Irregular and stranded contours without suspicious calcifications were also noted.
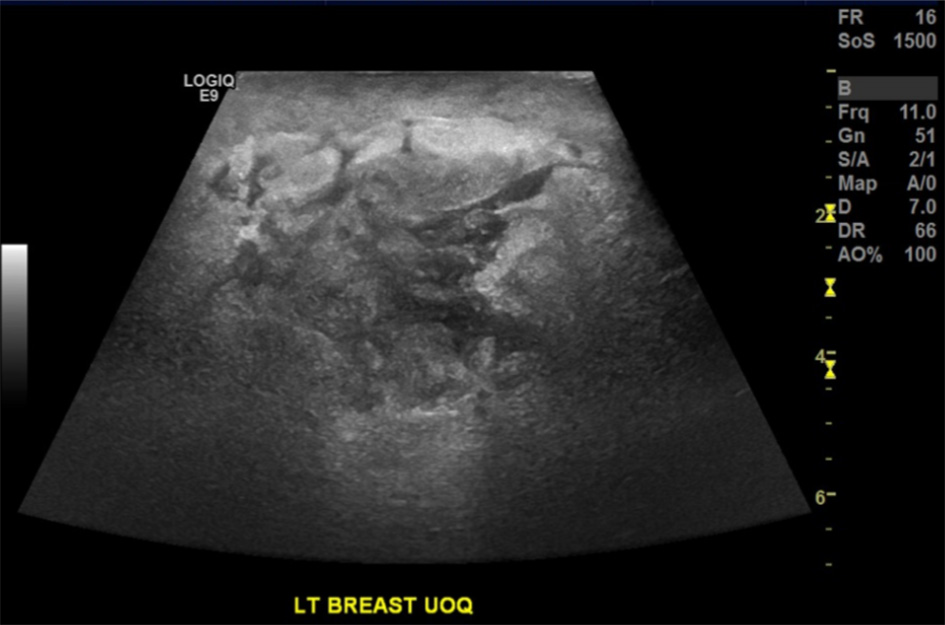
Figure 2. Ultrasound of the left breast demonstrating a lobulated, heterogeneous, hypoechoic mass lesion measuring 31 × 17 × 21 mm with accompanying distortion of the surrounding structures.

Figure 3. Clinical image of the left breast with a large wound containing central necrosis with surrounding purulent discharge and accompanying erythema extending to the nipple.
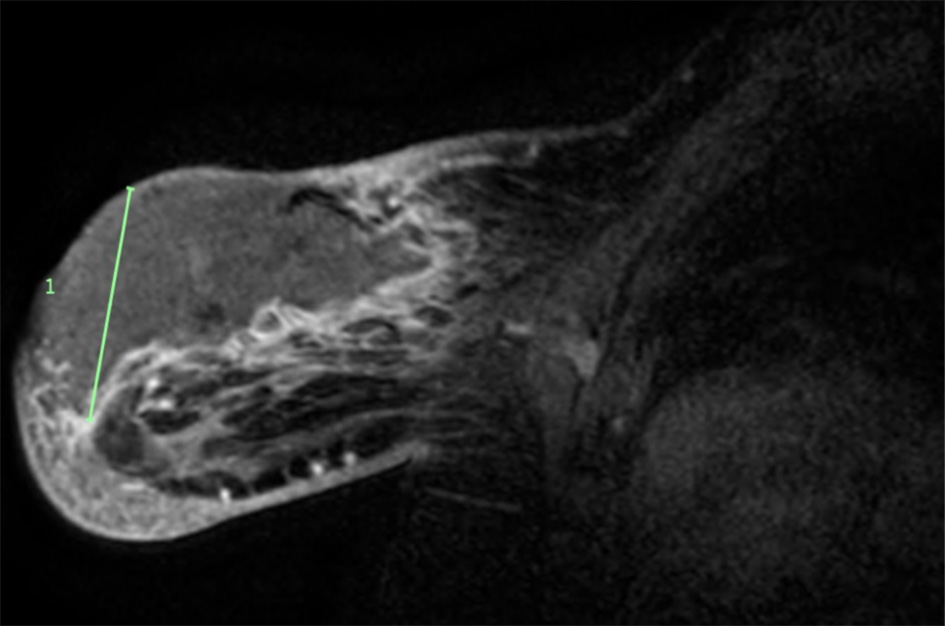
Figure 4. MRI of the left breast with a large collection, measuring100 × 40 × 60 mm. MRI features were in keeping with a large abscess with accompanying feature of skin breakdown and necrosis. MRI: magnetic resonance imaging.

Figure 5. Clinical image of left breast 2 weeks post debridement, with resolution of the infection and healthy granulation tissue in the base of the wound.
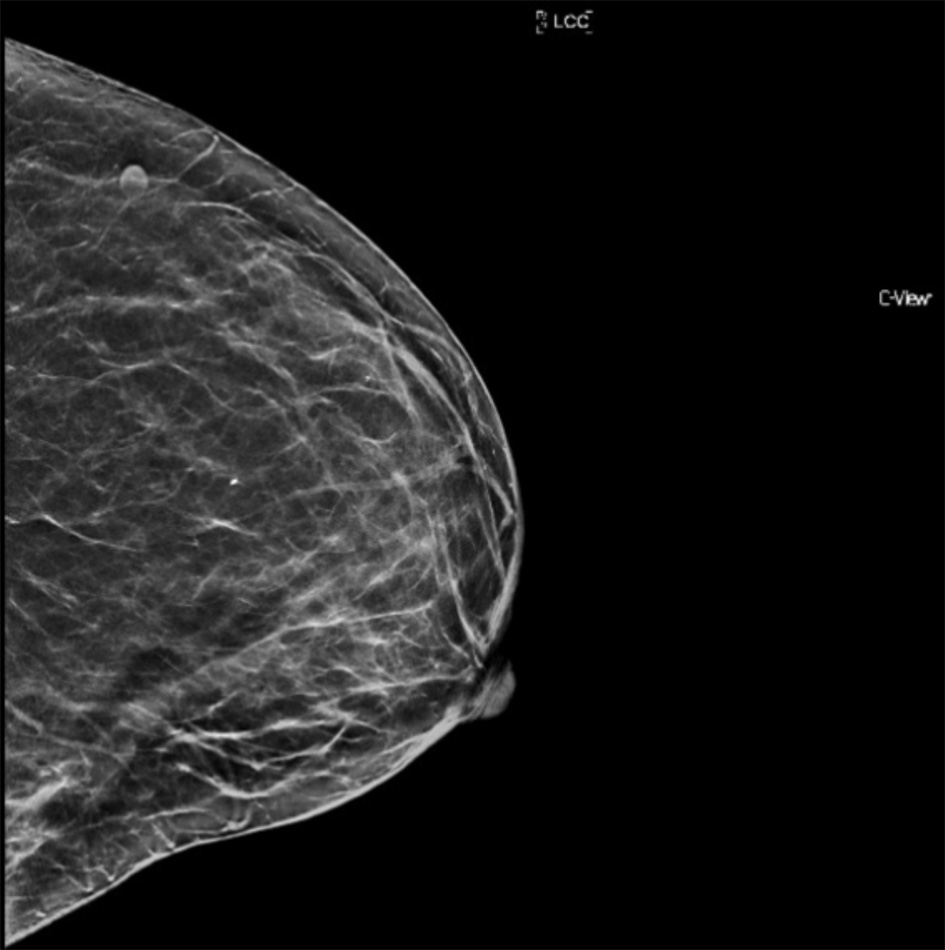
Figure 6. Follow-up mammogram (cranio-caudal view) 6 months post infection demonstrating almost complete resolution of previously visualized lesion.