Figures
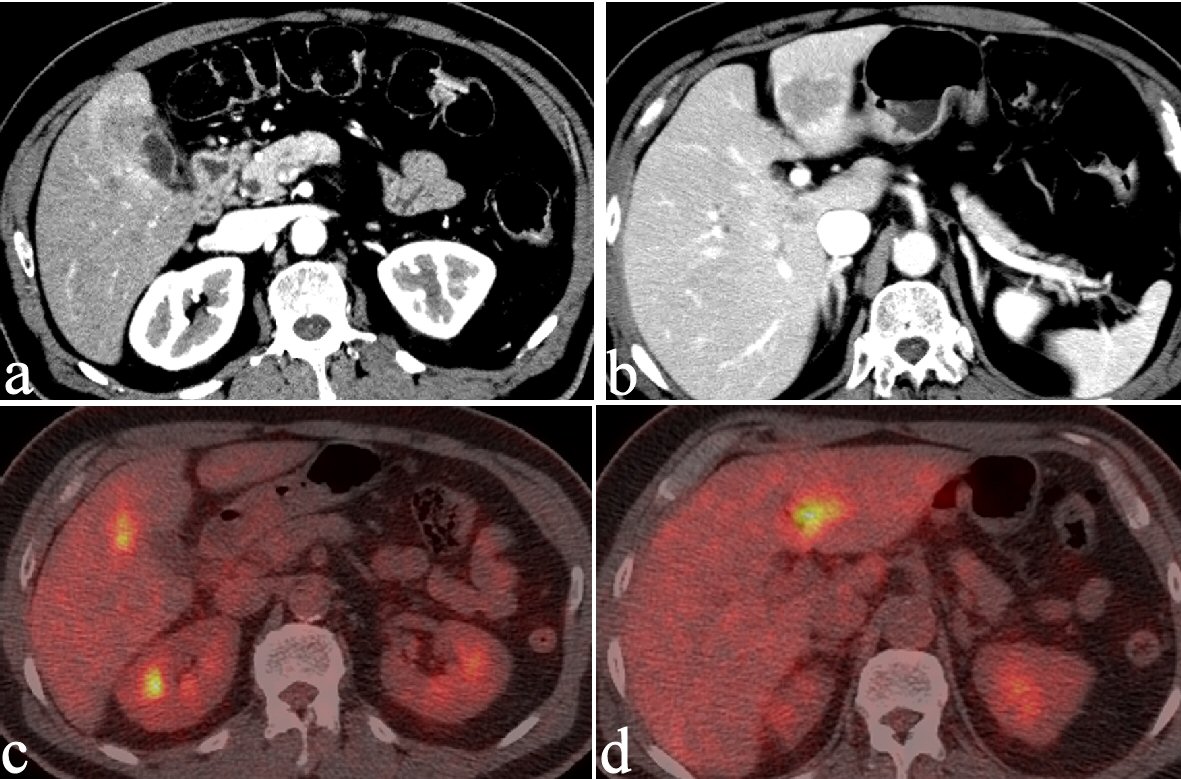
Figure 1. CT reveals an irregularly thickened GB wall showing an indistinct boundary with the neighboring liver (a) and an irregular, ring-enhancing, hypointense area in the left lobe of the liver (b). Both lesions show FDG accumulation on PET (c and d).
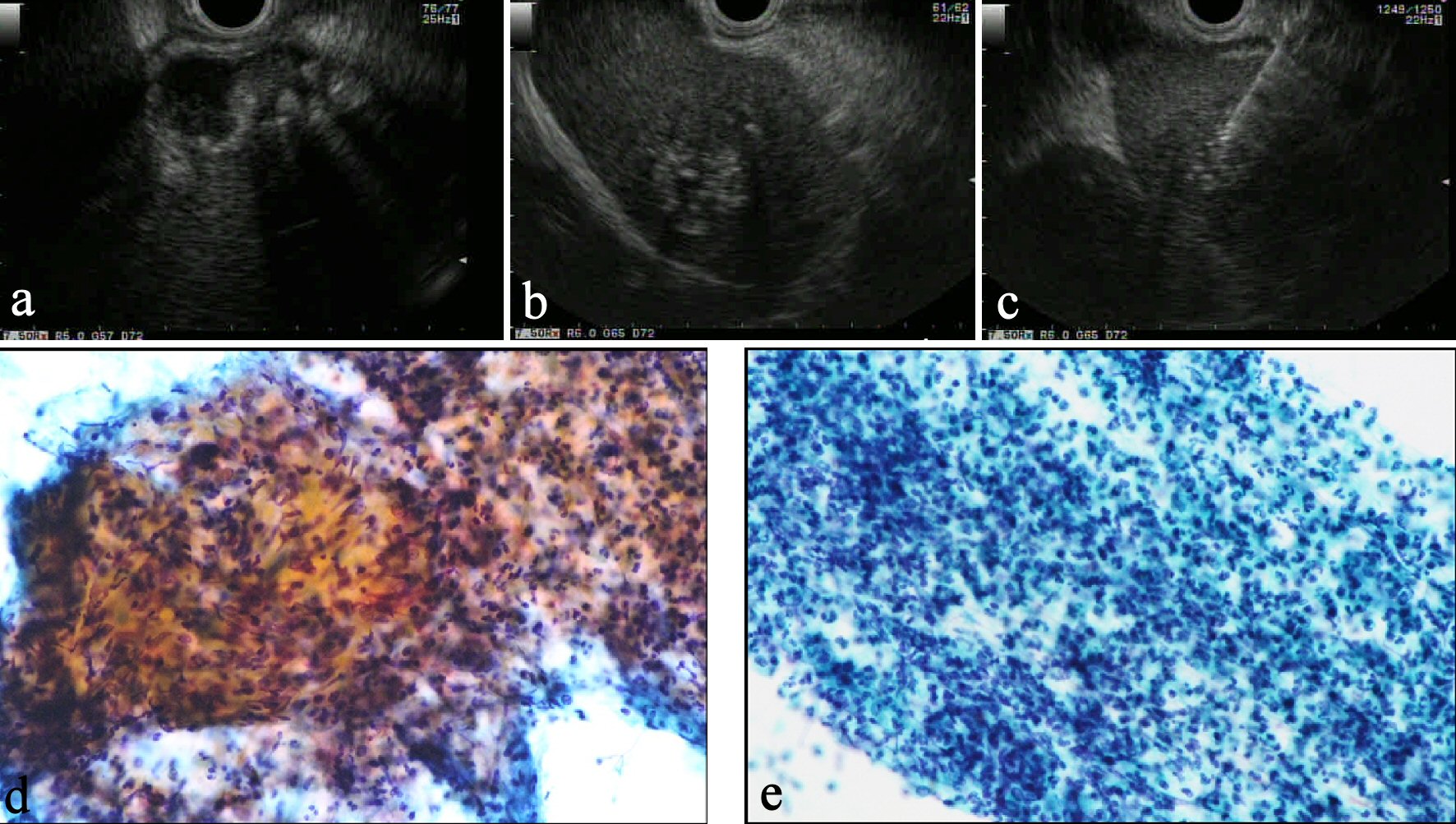
Figure 2. (a) On EUS, a Rokitansky-Aschoff sinus with stones is seen in the GB wall and the border between the GB and liver is unclear. (b) The mass in the left lobe is visualized as an aggregation of highly echoic spots. (c) EUS-FNA reveals typical inflammatory cells from both the liver mass (d) and GB wall (e), suggesting these lesions were not malignant disorder.
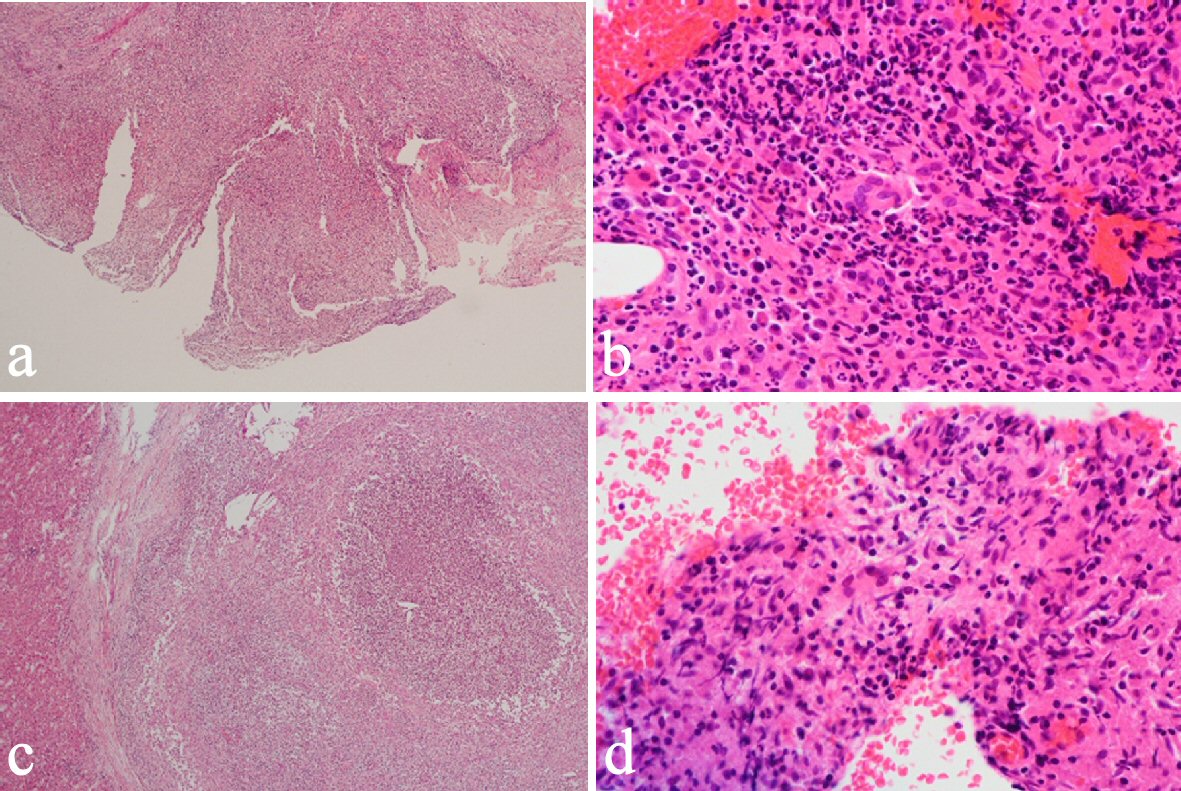
Figure 3. Cholecystectomy and liver lateral sectional resection showed foam cells and multinucleated giant cells with xanthogranulomatous inflammation in the GB wall (a, b) and similar phenomena in a nearby bile duct in the liver (c, d).
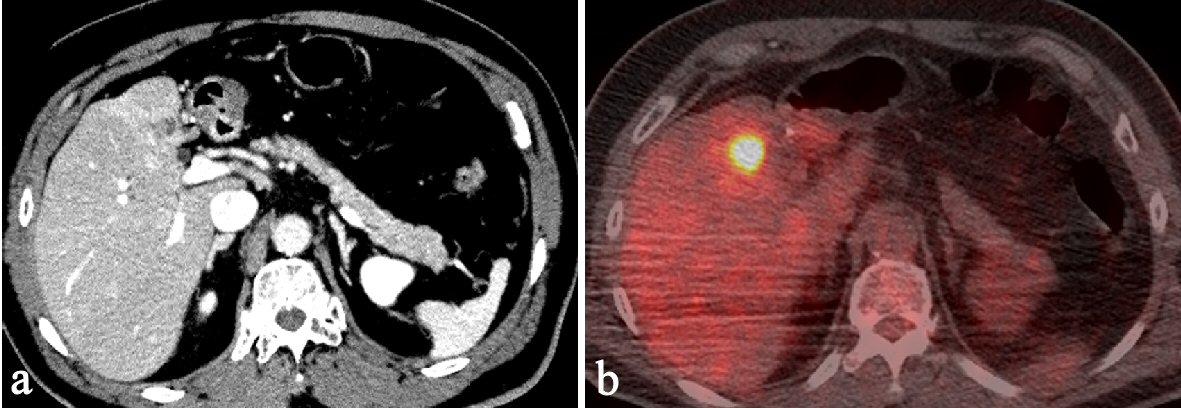
Figure 4. Ten months after first surgery, follow-up CT shows a new, irregular mass in the liver medial section. The mass shows delayed enhancement and accumulation of FDG on PET.
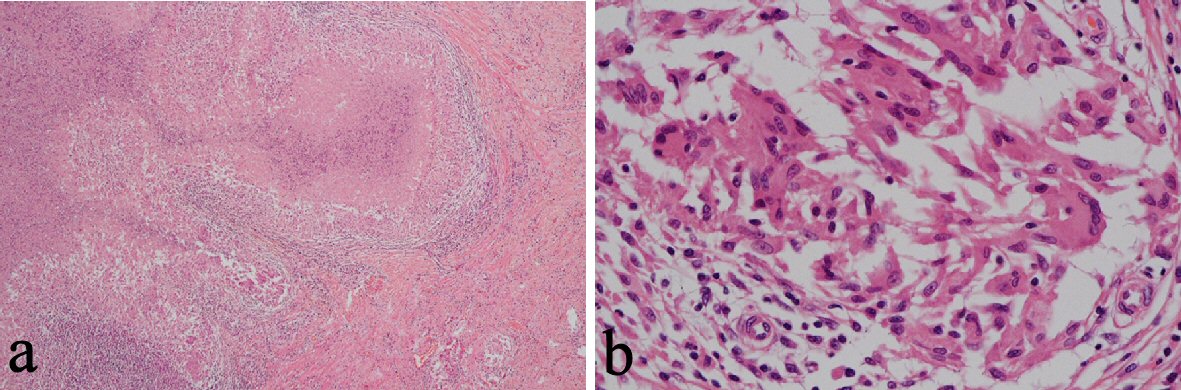
Figure 5. Following liver medial sectional resection, pathological examination revealed granulomatous inflammation, multinucleated giant cells and neutrophilic infiltration with fibrosis around a bile duct (a, b).