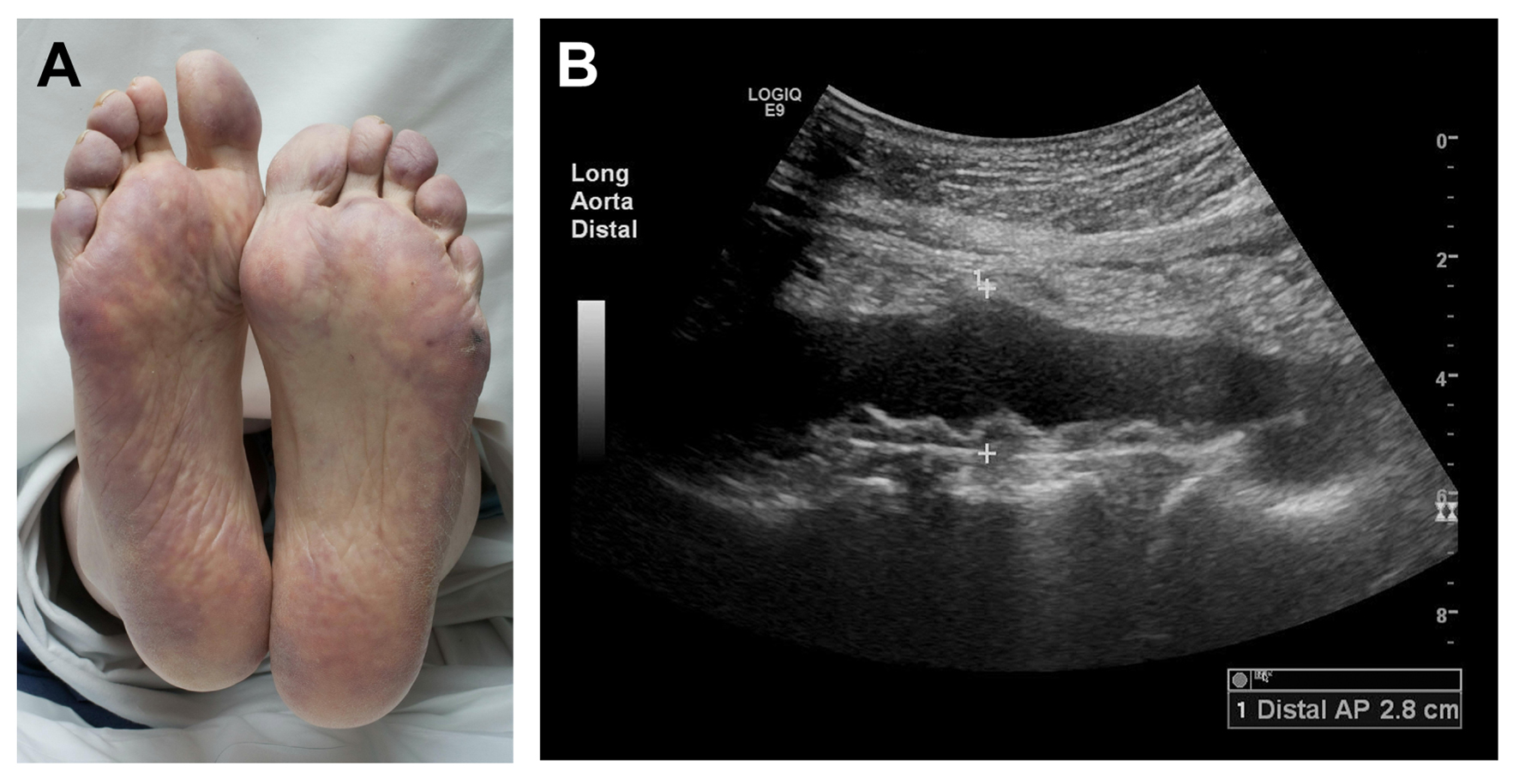
Figure 1. Ischemic skin manifestations of cholesterol embolization syndrome. (A) Marked purplish discoloration of plantar surfaces (livedo reticularis) and pallor and cyanosis of the toes, indicating acute loss of perfusion, several weeks after percutaneous intra-arterial intervention in a patient with (B) severe atherosclerosis of the thoracoabdominal aorta.
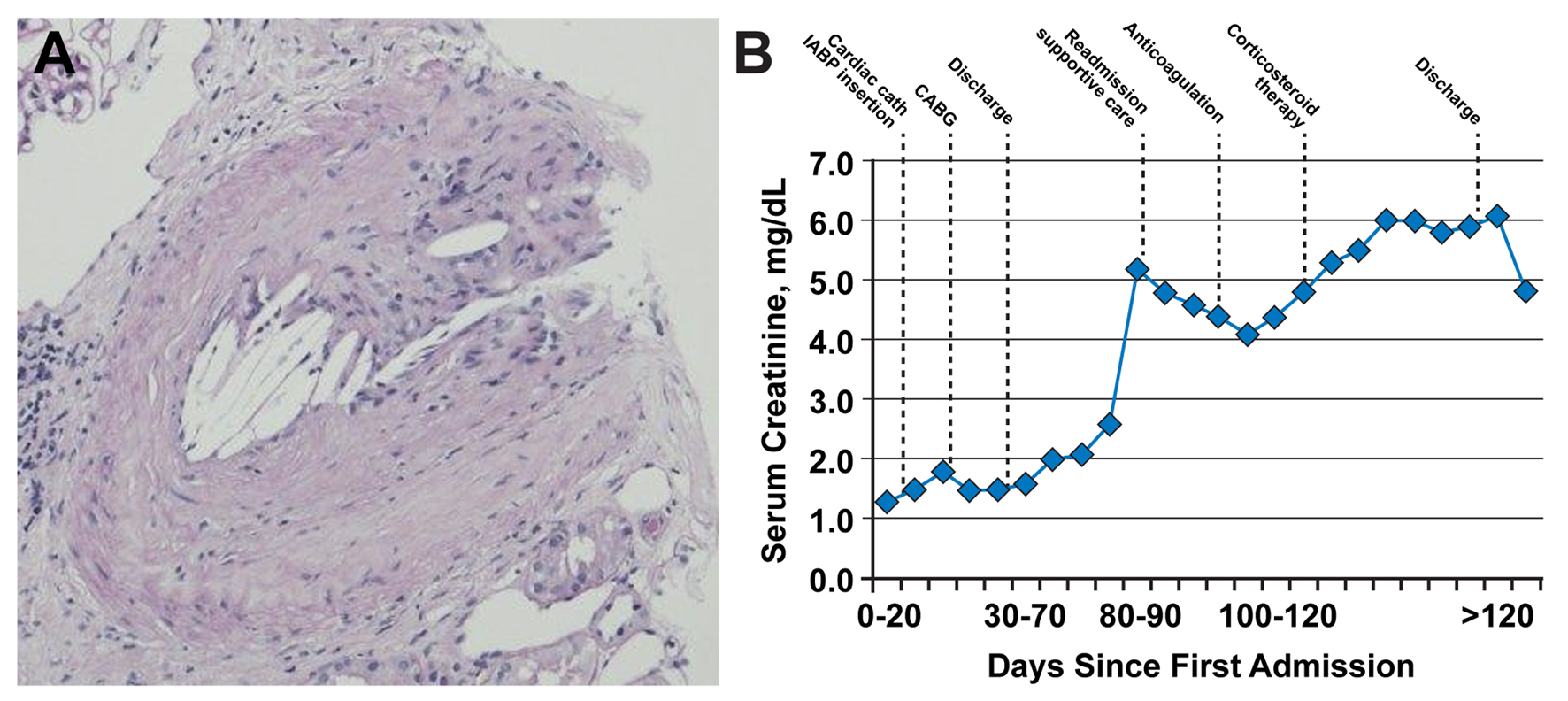
Figure 2. Renal biopsy results. (A) Occlusion of a branch renal artery by cholesterol emboli (hematoxylin and eosin, original magnification, × 100). Evidence of dissolved cholesterol crystals is represented by needle-shaped cholesterol clefts. (B) Time course of serum creatinine values in the days following initial vascular insult. Graph shows initial steady increase of serum creatinine and initial improvement with supportive care (mainly, intravenous fluid hydration), followed by worsening after initiation of anticoagulation, with subsequent stabilization and improvement after initiation of corticosteroid therapy. CABG: coronary artery bypass grafting; cath: catheterization; IABP: intra-aortic balloon pump.