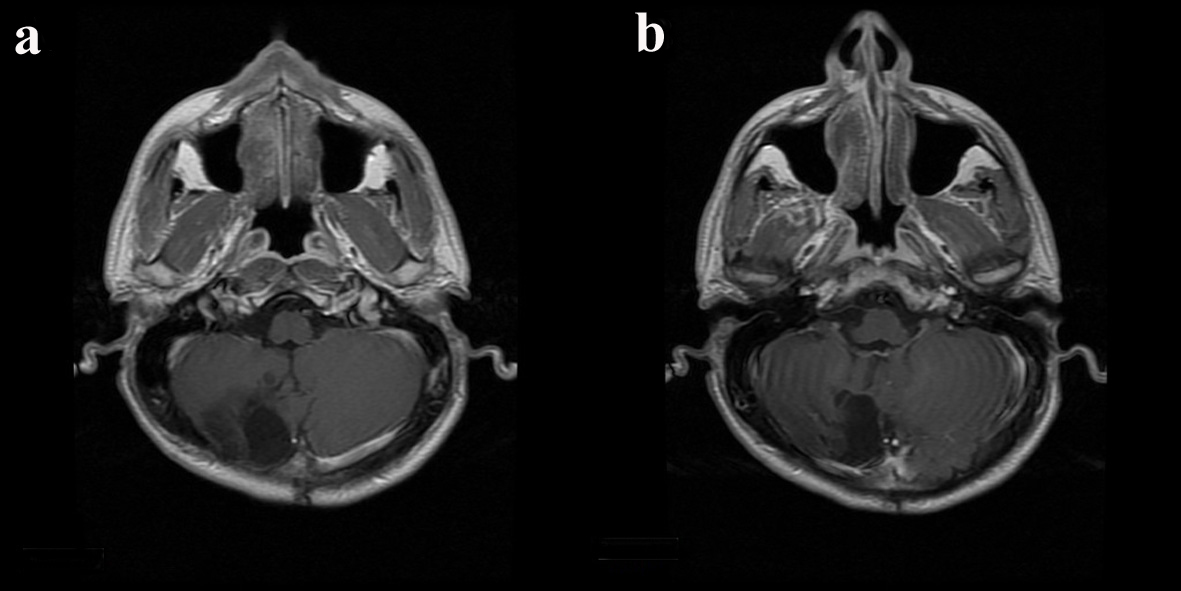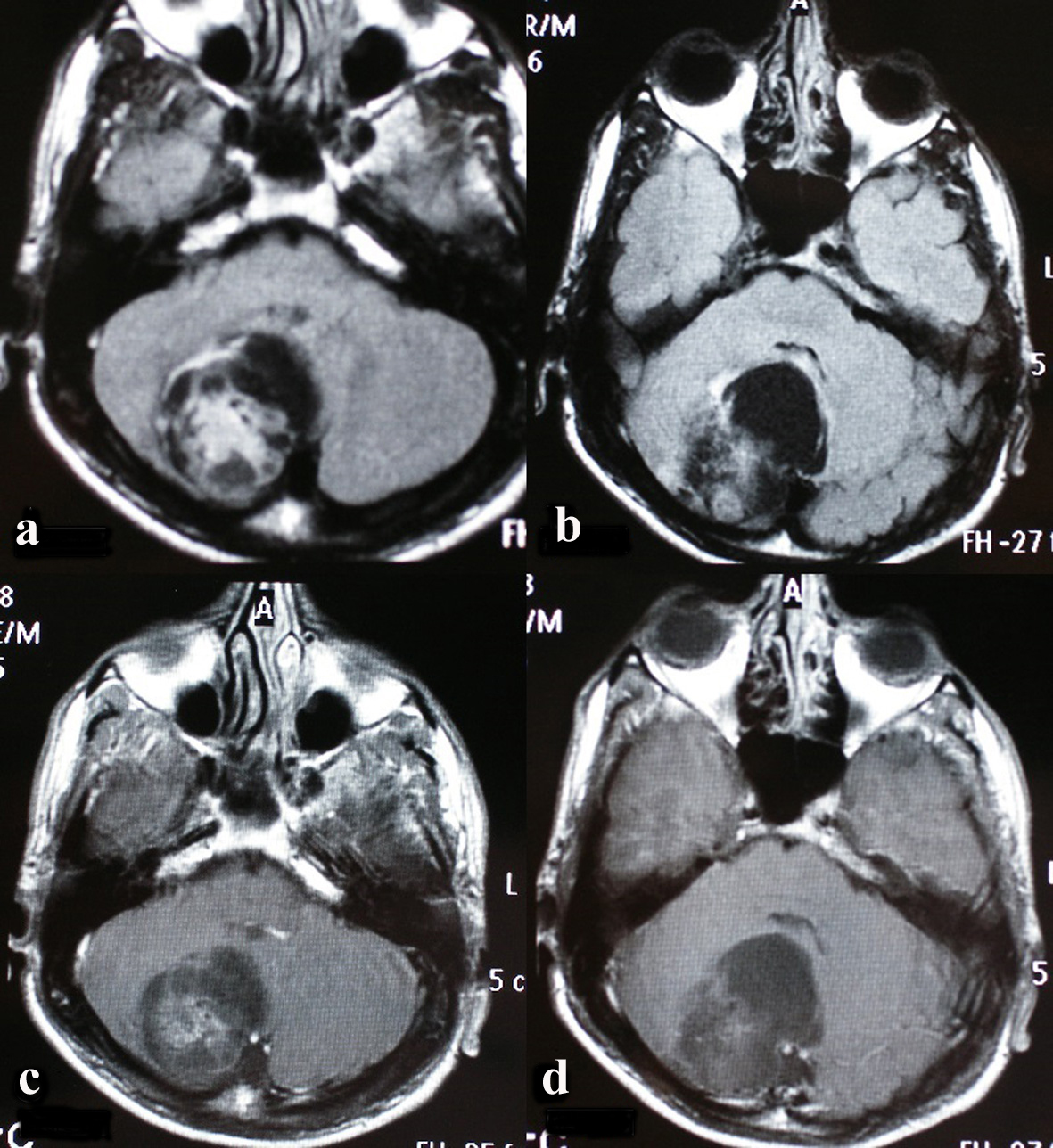
Figure 1. On the axial plan, on the fluid attenuated inversion recovery (FLAIR) incisions (a, b), a 4.5 × 4 × 4 cm expansile cystic lesion with solid components on the right cerebellar hemisphere next to the fourth ventricle is seen (c, d).
| Journal of Medical Cases, ISSN 1923-4155 print, 1923-4163 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Med Cases and Elmer Press Inc |
| Journal website http://www.journalmc.org |
Case Report
Volume 5, Number 5, May 2014, pages 304-307
Rosette-Forming Glioneuronal Tumor That Did Not Recur for Six Years: A Rare Case Report
Figures