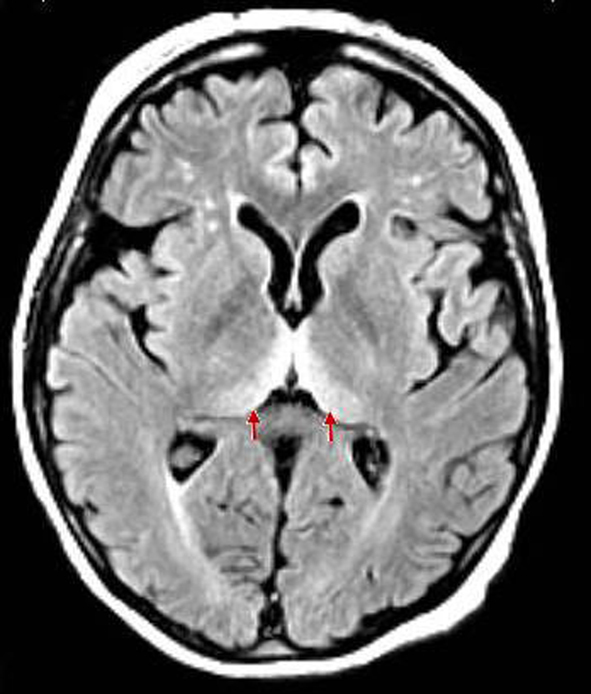
Figure 1. Clear findings for bilateral hyperintensities of the posterior thalamus relative to the signal intensity of the anterior putamen (pulvinar sign).
| Journal of Medical Cases, ISSN 1923-4155 print, 1923-4163 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Med Cases and Elmer Press Inc |
| Journal website http://www.journalmc.org |
Case Report
Volume 4, Number 11, November 2013, pages 765-768
Pulvinar Sign in Sporadic Creutzfeldt-Jakob Disease: Exploring the Diagnostic Modalities of Prion Diseases
Figure
Table
| Probable sCJD | Case | Suspected vCJD | |
|---|---|---|---|
| Other shared criteria include: alternative diagnosis ruled out by routine investigations. No history of iatrogenic exposure. No evidence of familial form of TSE. Duration of the disease greater than 6 months but less than 2 years. | |||
| Age | - | 71 | < 55 years old (current age or age of death) |
| Clinical features | Rapidly progressive dementia & (2/4): 1: myoclonus, 2: visual or cerebellar signs, 3: pyramidal/extrapyramidal signs, 4: akinetic mutism | Rapidly progressive dementia, visual and cerebellar signs, pyramidal signs, akinetic mutism, early psychiatric symptoms, dysesthesia changes, gait ataxia | Progressive neuropsychiatric disorder & (4/5): 1: early psychiatric symptoms, 2: persistent painful sensory symptoms, 3: ataxia, 4: myoclonus/chorea/dystonia, 5: dementia |
| Laboratory testing | (1/3): 1: typical sCJD EEG abnormality: periodic sharp bursts, 2: +14-3-3 CSF assay, 3: typical sCJD MRI abnormalities: signal hyperintensity in the basal ganglia and cortical ribboning (DWI & FLAIR) | EEG not diagnostic of sCJD MRI: pulvinar sign: symmetrical high diffusion signal in bilateral pulvinar thalami +14-3-3 CSF assay | EEG not diagnostic of sCJD MRI: pulvinar sign: symmetrical high diffusion signal in bilateral pulvinar thalami. Posterior thalami involvement (FLAIR, DWI & T2) |