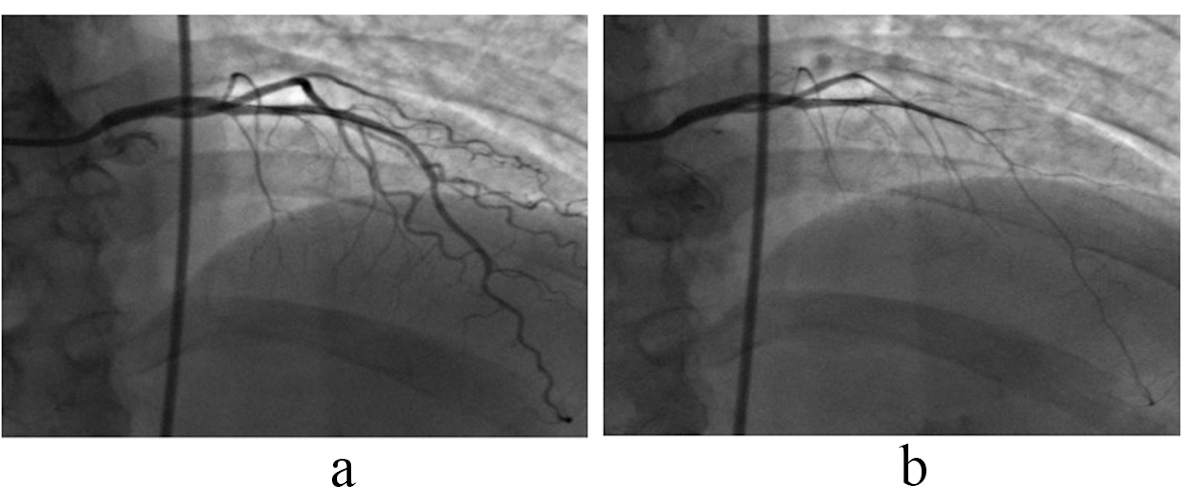
Figure 1. Angiogram of left anterior descending (LAD): There was 60% reduction in LAD diameter measured by Quantitative Coronary Angiography (QCA) following intracoronary injections of 10-4 acetylcholine (b) from baseline (a) indicating coronary endothelial dysfunction (normal response is vasodilatation). Arrows indicate position of tip of the Doppler flow wire.