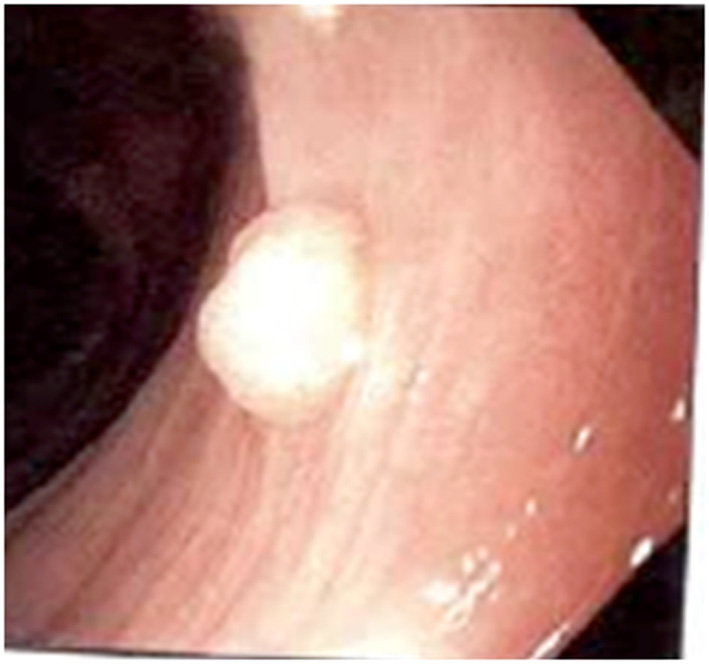
Figure 1. Olympus video gastroscope shows a 0.8 cm polyp in the mid portion of the interposed colon.
| Journal of Medical Cases, ISSN 1923-4155 print, 1923-4163 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Med Cases and Elmer Press Inc |
| Journal website http://www.journalmc.org |
Case Report
Volume 6, Number 5, May 2015, pages 188-193
Tubular Adenomatous Polyp in a Colon Interposition: A Case Report and Review of Literature
Figures

Table
| References | Age | Gender | Comorbidities | Indication for esophagectomy | Histology | Time from esophagectomy (years) | Treatment | Recommendations post-treatment |
|---|---|---|---|---|---|---|---|---|
| GERD: gastroesophageal reflux disease; Htn: hypertension; DMII: diabetes mellitus type 2; SCC: small cell cancer; s/p: status post; EGD: esophagogastroduodenoscopy. | ||||||||
| [2] | 80 | M | - | esophageal squamous cell carcinoma | Adenocarcinoma in a tubular adenoma | 14 | Endoscopic submucosal dissection | Upper endoscopic screening within 1 year |
| [3] | 59 | F | Gastric ulcer perforation | Anastomotic stricture | Adenocarcinoma | 56 | Surgical resection | - |
| [21] | 65 | M | Hiatal hernia, ulcerated esophagus | Recurrent esophageal stricture | Tubular adenoma | 15 | Polypectomy | Repeat EGD and colonoscopy |
| [22] | 64 | M | - | Benign esophageal stricture | Adenocarcinoma from a villous adenoma | 20 | Surgery | - |
| [23] | 60 | M | GERD, Gastric ulcer | Benign esophageal stricture | Adenocarcinoma | 40 | Surgical resection | - |
| [24] | 60 | M | Colorectal cancer, Inflammatory bowel disease | Esophageal stricture | Invasive adenocarcinoma | 30 | Chemotherapy with 5-fluorouracil | Upper endoscopic screening every 5 years |
| [25] | 78 | M | Carcinoma of the gastric cardia, prostate cancer, diverticulosis | Necrosis and gangrene of the esophagogastric anastomosis | Adenocarcinoma | 10 | Surgical resection | - |
| [26] | 11 | M | - | Esophageal stricture | Juvenile polyp | 8 | Polypectomy | - |
| [27] | 68 | M | - | - | Adenocarcinoma | 12 | Surgical resection | - |
| [28] | 63 | F | - | Esophageal perforation | Tubular adenoma with low grade dysplasia | 8 | Polypectomy | Repeat EGD screening at 5 years |
| [28] | 65 | F | - | Persistent fistula following esophagectomy for carcinoma | Tubulovillous adenoma with low grade dysplasia | 3 | Polypectomy | Repeat EGD at earlier stage due to high risk of malignancy |
| [29] | 64 | M | Htn, DMII, GERD | Persistent reflux symptoms post Roux-en-Y surgery | Tubular adenoma | 7 | Polypectomy | - |
| [30] | 72 | M | GERD | Epidermoid carcinoma of the esophagus | Adenocarcinoma | 9 | Chemotherapy with 5-flourouracil | Patient deceased due to progression of tumor |
| [31] | 65 | M | Perforated duodenal ulcer | Esophageal cancer | Sessile polyp/adenomatoid polpus | 6 | Polypectomy | Repeat EGD 5 years later revealed malignant lesion |
| [32] | 48 | F | - | Epidermoid carcinoma | Adenocarcinoma in a villous adenoma | 2 | Surgical resection and a new cologastrostomy | Esophagram every 6 months |
| [33] | 75 | F | - | Posterior SCC s/p pharyngolaryngectomy | Adenocarcinoma | 20 | Surgical resection of the colon graft | - |
| [14] | 66 | M | Barrett’s esophagus | Recurrent esophageal adenocarcinoma s/p proximal gastrectomy and distal esophagectomy | Adenocarcinoma | 2 | Surgical resection | Regular follow up |
| [34] | 51 | M | - | Benign esophageal stricture | Adenocarcinoma | 11 | - | - |
| [35] | 79 | M | - | Esophageal cancer | Adenocarcinoma | 30 | Chemotherapy | - |
| [36] | 57 | M | - | Alkaline corrosive injury of the esophagus | Adenocarcinoma | 37 | Surgical resection | - |
| [37] | 79 | M | - | Esophageal adenocarcinoma | Adenocarcinoma | 7 | Surgical resection | - |
| [38] | 65 | M | - | - | Tubular adenoma | 1 | Polypectomy | Routine follow-up |
| Our case | 59 | M | Diverticulitis, hypoglycemia, Barrett’s esophagus | Barrett’s esophagus with high grade dysplasia | Tubular adenoma | 6 | Polypectomy | EGD survaillence in 3 yrs |