








| Journal of Medical Cases, ISSN 1923-4155 print, 1923-4163 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Med Cases and Elmer Press Inc |
| Journal website http://www.journalmc.org |
Case Report
Volume 1, Number 3, December 2010, pages 111-113
A Unique Case of Posterior Sternoclavicular Joint Dislocation With Fracture of Transverse Process of First Thoracic Vertebrae
Deepak Doshia, c, Ravindranadha R. Kalakotib
aLogan Hospital, Meadowbrook, QLD, Australia
bChesterfield Royal Hospital, Chesterfield, UK
cCorresponding author: Emergency Department, Logan Hospital, Cnr Armstrong and Loganlea roads, Meadowbrook, QLD 4131, Australia
Manuscript accepted for publication November 17, 2010
Short title: Posterior Sternoclavicular Joint Dislocation
doi: https://doi.org/10.4021/jmc82w
| Abstract | ▴Top |
Sternoclavicular joint injuries are rare. Mechanism of injury holds a significant clue along with clinical features. Fracture of transverse process of first thoracic vertebra can be associated with sternoclavicular joint injury. Sports related injuries can be of complex nature and, if undetected at an early stage, can have a significant impact for patient in future. We report a unique case of posterior sternoclavicular dislocation with a fracture of transverse process of first thoracic vertebrae.
Keywords: Sternoclavicular; Dislocation; Vertebrae
| Case Report | ▴Top |
A 15 years old boy presented to Emergency department following injury to his chest while playing rugby. He was tackled in the game and then he fell to the ground on his chest. Two other players fell on his back. He was brought in by ambulance. He complained of pain in his chest without any difficulty in breathing.
On initial assessment, his airway examination was clear and he was able to speak full sentences. His respiratory rate was 24 breaths per minute and oxygen saturation was 100% on room air. He had bilateral good air entry. His respiration was shallow which he attributed to pain. He was tachycardic at 120/minute and his blood pressure was 106/74 in his right and 110/76 in his left upper limb. His pain score was 6 out of 10 on visual analogue scale.
Further examination suggested that he was tender on his left sternoclavicular (SCL) joint area with minimal swelling of soft tissue. His left shoulder examination revealed that he had restricted flexion and abduction due to pain. There was no localized pain at his shoulder joint. Distal vascular examination was normal on both his upper limbs. There was no neurological deficit.
He was given analgesics, and a chest and a left shoulder x-rays were obtained. His chest x-ray showed that he had a transverse fracture of his first thoracic vertebrae (Fig. 1). His shoulder was normal on x-ray examination. Sternoclavicular joint was poorly visualized on x-ray. He was referred to an orthopaedic surgeon. He had no significant medical history. A computerized tomogram of his chest showed that he had posterior dislocation of his clavicle and a transverse fracture of his first thoracic vertebrae. He also had a spiral fracture of his lateral clavicle (Fig. 2).
 Click for large image | Figure 1. Plain x-ray film showing fracture of transverse process of first thoracic vertebrae. Clavicle dislocation is often masked due to anatomical reasons in the plain films. |
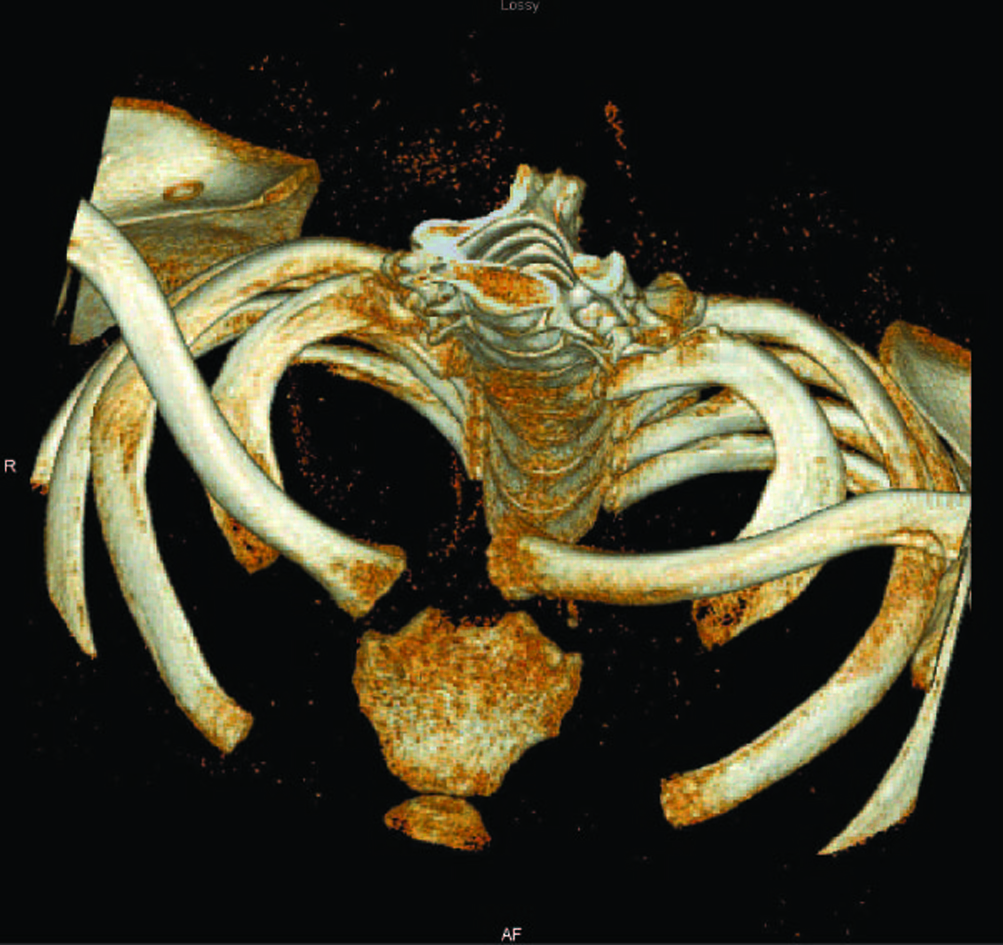 Click for large image | Figure 2. Computed reconstructed tomogram showing posterior dislocation of left sternoclavicular joint with a spiral fracture of the lateral end of clavicle. |
An unsuccessful attempt was made at closed reduction with image intensifier. A skin crease incision was made over the sternoclavicular joint. Physeal injury with posterior dislocation of clavicle and Salter Harris type I fracture at the medial end of clavicle were identified. Drill holes through the medial metaphysis of clavicle were sutured through the epiphysis. Check images on operation table were satisfactory.
His recovery was uneventful at six weeks follow-up. He was given Codman exercise program by physiotherapist for his functional rehabilitation. He had complete functional recovery at further follow-up at three months.
| Discussion | ▴Top |
Posterior dislocation of sternoclavicular joint is a rare injury [1, 2].
The authors believe that this is the first reported case of posterior dislocation of SCL with fracture of transverse fracture of first thoracic vertebra (T1).
The reported cases of SCJ dislocations are anterior, posterior and atraumatic types [3] (Table 1). However, there is no report of any of the SCL dislocation diagnosed along with and as a clue from the fracture of the transverse process of T1. Most described posterior dislocations have resulted as indirect trauma with significant intra-thoracic injuries [4, 5]. This case is unusual in that there was no major intra-thoracic organ involvement.
 Click to view | Table 1. Causes of Sternoclavicular Joint Dislocation |
SCL joint is very close to the major vital structures including great vessels of the neck and thorax, lung and the pleura, brachial plexus, trachea, and esophagus [6, 7].
It was clear from our case that posterior dislocation of SCL joint is often a difficult diagnosis both clinically and even from plain x-ray films [8-11]. In any such significant mechanism of injury, emergency physicians should look for a tell-tale sign such as a transverse fracture of the T1 or spiral fracture of the clavicle. We have called this a ‘Doshi’s sign’ for further investigation for the diagnosis of posterior dislocation of SCL.
Posterior dislocation should always be surgically reduced, as this is a very unstable joint with minimum ligament support and there is high risk of impingement on the visceral structures. There are significant chances of even late neurovascular complications [12].
Closed reduction would warrant a regular follow-up for months to look for any delayed complications. Open reduction has advantage of providing support with artificial strengthening materials such as nylon or steel clips.
In conclusion, a chest x-ray suggestive of transverse fracture of first thoracic vertebra indicates a significant injury. Further evaluation of thorax and spine should be performed specifically looking for sternoclavicular joint dislocation.
Conflict of Interest
The authors declare no conflict of interest.
| References | ▴Top |
- Hoekzema N, Torchia M, Adkins M, Cassivi SD. Posterior sternoclavicular joint dislocation. Can J Surg 2008;51(1):E19-20.
pubmed - Jougon JB, Lepront DJ, Dromer CE. Posterior dislocation of the sternoclavicular joint leading to mediastinal compression. Ann Thorac Surg 1996;61(2):711-713.
pubmed doi - Bicos J, Nicholson GP. Treatment and results of sternoclavicular joint injuries. Clin Sports Med 2003;22(2):359-370.
pubmed doi - Abdulla SR, Gandham SG. Posterior dislocation of sternoclavicular joint in a child. J Accid Emerg Med 1999;16(5):385.
pubmed - Rajaratnam S, Kerins M, Apthorp L. Posterior dislocation of the sternoclavicular joint: a case report and review of the clinical anatomy of the region. Clin Anat 2002;15(2):108-111.
pubmed doi - Doss A, Lang IM, Roberts I, Bell MJ, Smith TW. Posterior sternoclavicular joint dislocation in children-role of spiral computed tomography. Pediatr Emerg Care 2005;21(5):325-326.
pubmed doi - Kaufman RL. Manipulative reduction and management of anterior sternoclavicular joint dislocation. J Manipulative Physiol Ther 1997;20(5):338-342.
pubmed - Chakarun CJ, Wolfson N. Adult male with right shoulder pain. Posterior sternoclavicular joint dislocation. Ann Emerg Med 2009;53(6):714, 745.
pubmed - Fenig M, Lowman R, Thompson BP, Shayne PH. Fatal posterior sternoclavicular joint dislocation due to occult trauma. Am J Emerg Med 2010;28(3):385 e385-388.
pubmed - Pearson MR, Leonard RB. Posterior sternoclavicular dislocation: a case report. J Emerg Med 1994;12(6):783-787.
pubmed doi - Peng C, Sun DC, Li JG, He CG, Hu CL. [Treatment of anterior dislocation of sternoclavicular joint with Kirschner wire minimally invasive fixation]. Zhongguo Gu Shang 2010;23(2):151-153.
pubmed - Laffosse JM, Espie A, Bonnevialle N, Mansat P, Tricoire JL, Bonnevialle P, Chiron P, et al. Posterior dislocation of the sternoclavicular joint and epiphyseal disruption of the medial clavicle with posterior displacement in sports participants. J Bone Joint Surg Br 2010;92(1):103-109.
pubmed doi
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Medical Cases is published by Elmer Press Inc.