*Average article statistics from the last 12 months data
COVID-19 RESEARCH
The COVID-19 outbreak presents the unprecedented challenge for world public and medical practitioners and health care providers, the post COVID-19 condition (or long COVID) includes long term symptoms which may persist for months or years after SARS-CoV-2 infection. We will consider submissions related to all aspects of COVID-19 and Long COVID, and process the manuscripts in priority.
Journal of Medical Cases, ISSN 1923-4155 print, 1923-4163 online, Open Access
Article copyright, the authors; Journal compilation copyright, J Med Cases and Elmer Press Inc
Journal website http://www.journalmc.org
Case Report
Volume 8, Number 7, July 2017, pages 215-218
Laparoscopic Enucleation of Schwannoma Masquerading as a Leiomyoma
Howard S. Fana, b, Ahmed A. Rahmana, Michael L. Talbota
aDepartment of Surgery, University of New South Wales, St George Hospital, Kogarah, NSW 2217, Australia bCorresponding Author: Howard S. Fan, Department of Surgery, University of New South Wales, St George Hospital, Kogarah, NSW 2217, Australia
Manuscript submitted April 6, 2017, accepted April 24, 2017 Short title: Laparoscopic Enucleation of Schwannoma doi: https://doi.org/10.14740/jmc2823w
We present a case, literature review, and video of a transabdominal laparoscopic enucleation of an esophageal schwannoma. A 53-year-old female with dysphagia was found to have a 23 × 27 mm mass in the lower esophagus, which was initially diagnosed as a leiomyoma on endoscopic ultrasound without biopsy. At the time of her laparoscopic enucleation 12 months later, the lesion had grown to 60 × 55 × 30 mm and was excised with a full-thickness segment of the esophageal wall, with closure of the resulting defect over a bougie. Postoperatively, the patient’s recovery was complicated by an esophageal leak which was successfully managed with endoscopic drainage. Esophageal schwannomas are rare esophageal lesions that have historically been treated with esophagectomy. Thoracoscopic or laparoscopic enucleations of smaller lesions have been more recently reported but larger lesions have usually required open surgery. Internally placed endoscopic drains have previously been shown to be a valid alternative to external drainage in patients with contained collections after resection surgery. They have the advantage of allowing patients to continue oral fluids during the recovery phase rather than relying on enteral or parenteral feeding. We propose that laparoscopic transabdominal enucleation of esophageal schwannoma with closure of the resulting full-thickness defect be considered as an organ and function sparing alternative for the management of large lower esophageal schwannomas. We further propose that contained leaks resulting from esophageal operations can successfully be managed with internal endoscopic drainage.
Esophageal schwannomas are rare esophageal lesions that have historically been treated with esophagectomy. Thoracoscopic or laparoscopic enucleations of smaller lesions have been more recently reported but larger lesions have usually required open surgery. We present a case, literature review, and video of a transabdominal laparoscopic enucleation of a 60 × 55 × 30 mm esophageal schwannoma which was initially diagnosed on endoscopic ultrasound as a leiomyoma.
A 53-year-old female, with no significant medical history, presented to hospital for investigation of dysphagia. An endoscopy was performed with the initial endoscopic ultrasound without biopsy revealing a 23 × 27 mm mass in the lower esophagus arising from the muscularis mucosa. This was diagnosed as a likely leiomyoma and the patient was booked on the waitlist for an elective laparoscopic enucleation on a 12 months priority. The patient had ongoing dysphagia but remained clinically well during this period.
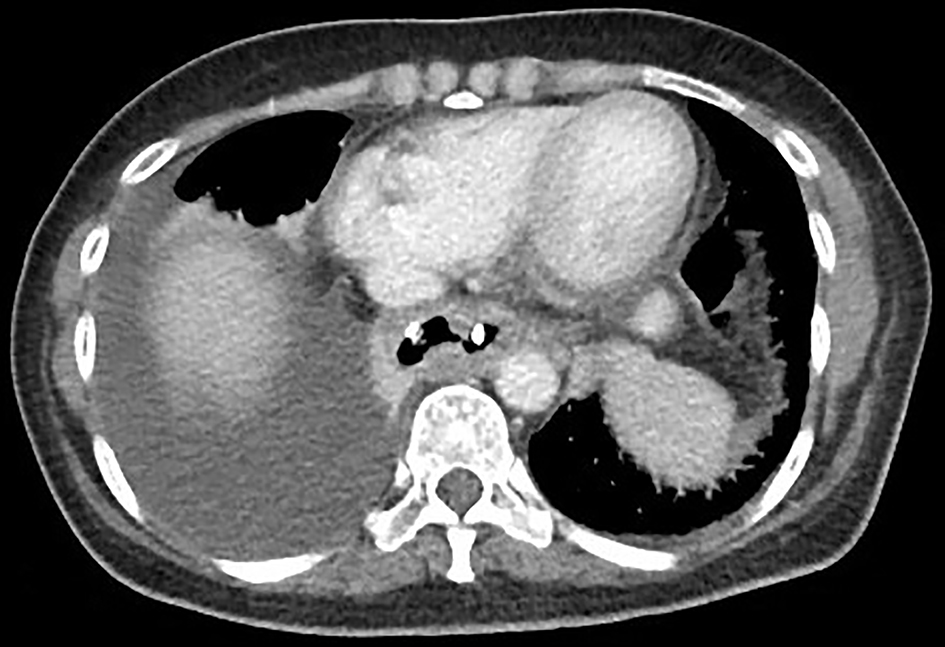
At the time of transabdominal laparoscopic enucleation, the lesion had grown to 60 × 55 × 30 mm, and a decision was made to continue with the planned procedure (Supplementary video 1, www.journalmc.org). While the tumor could be enucleated from the mediastinal structures, it could not be excised without creation of a 5 cm long mucosal defect. This defect was closed laparoscopically over on esophageal bougie and a surgical drain was placed. Postoperatively, the patient remained clinically well with stable blood chemistry and hematology result, apart from a raised C-reactive protein of 333 mg/L. An initial postoperative endoscopy did not reveal any abnormalities, and the patient was subsequently placed on oral feeds. In the following days oral feeds were observed in the external drains and an esophageal leak was confirmed on computed tomography (CT) and gastrografin swallow series (Fig. 1). The patient was initiated on bowel rest, intravenous antibiotics and taken back for endoscopy to manage the leak. The repeat endoscopy using a distal EMR cap to push the mucosa away provided a clearer image and revealed an esophageal defect at the apex of the suture-line. An internal 7 × 7 double J catheter was inserted through the defect via endoscopy. The external drain was subsequently removed and a repeat CT confirmed the endoscopically inserted drain in a satisfactory position with the distal end in the paraesophageal collection (Figs. 2 and 3). The patient was placed on a fluid diet the next day and completed 48 h of intravenous antibiotics before being discharged on day 3 on soft diet. She returned for endoscopic removal of drain at 7 weeks and has since remained well with no further complications.
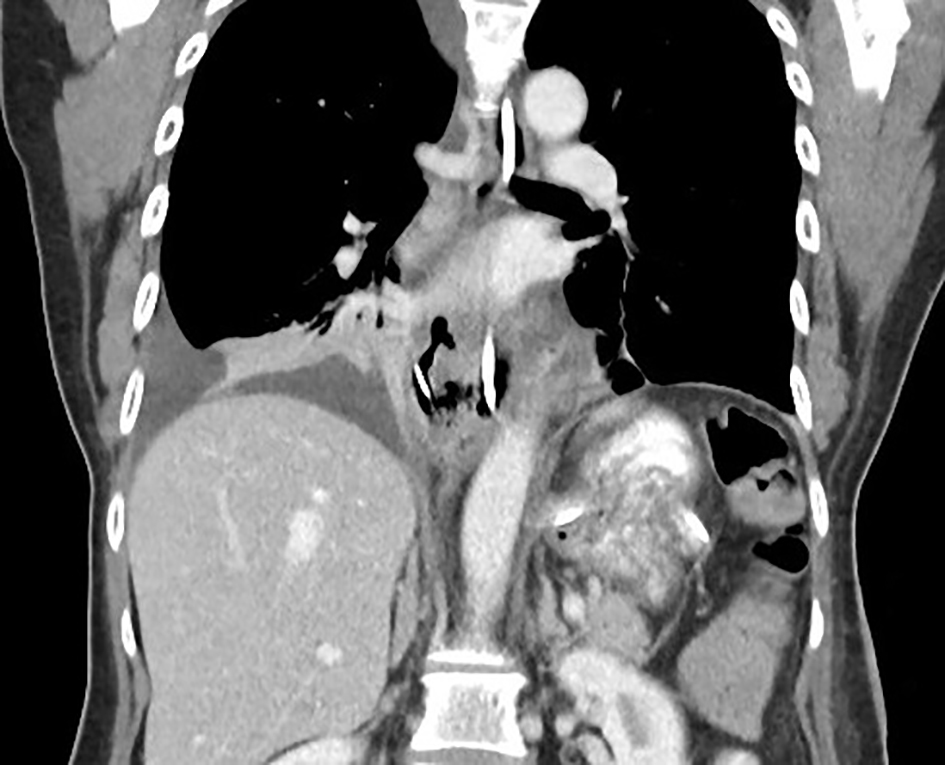
Figure 3. CT image, coronal view, showing double J catheter in esophagus traversing through the defect with distal end in the paraesophageal collection.
The most common benign intramural tumors of the esophagus are esophageal leiomyomas, which have an overall incidence of 0.1% and are typically located in the middle and lower thirds of the esophagus, and have historically been surgically managed through thoracotomy and enucleation of the lesion [1]. More recently, enucleation of esophageal tumors using minimally invasive thoracoscopic, laparoscopic and endoscopic techniques has been shown to be superior to open techniques in terms of reducing postoperative hospital stay, with no difference in operative time, intraoperative complications, or recurrence [2].
Esophageal schwannomas are exceedingly rare with only a handful of cases reported in the literature [3]. A literature review performed for the past decade, 2005 - 2015, revealed a total of 21 cases of which two cases were of concurrent esophageal schwannomas [3-20]. The surgical approaches to these include four thoracoscopic, six thoracotomy, five cervical approaches, and five esophagectomies or partial esophagectomies. To the best of our knowledge, there were no reported cases treated by a transabdominal laparoscopic approach. Only two of the reported cases were of esophageal schwannomas in the lower esophagus and both were enucleated with thoracotomy approaches (Table 1) [3-20].
Table 1. Existing Literature on Schwannoma Size, Location and Surgical Approach for Removal of the Lesion [3-20]
The management of postoperative esophageal leaks with endoscopically placed internal drains is a valid alternative to external drains as demonstrated by Talbot, Yee and Saxena (2015) who have successfully treated their patients with localized collections after esophagogastrectomies and gastrectomies with internal drainage [21]. They have the advantage of allowing patients to continue oral fluids during the recovery phase rather than relying on enteral or parenteral feeding. Our use of internal drainage in preference to external drainage of this patient allowed for easier drainage management and an earlier discharge from hospital.
Conclusion
We propose that laparoscopic transabdominal enucleation of esophageal schwannomas with closure of the resulting full-thickness defect be considered as an organ and function sparing alternative for the management of large lower esophageal schwannomas. We further propose that contained leaks resulting from esophageal operations can successfully be managed with internal endoscopic drainage.
Mutrie CJ, Donahue DM, Wain JC, Wright CD, Gaissert HA, Grillo HC, Mathisen DJ, et al. Esophageal leiomyoma: a 40-year experience. Ann Thorac Surg. 2005;79(4):1122-1125. doipubmed
von Rahden BH, Stein HJ, Feussner H, Siewert JR. Enucleation of submucosal tumors of the esophagus: minimally invasive versus open approach. Surg Endosc. 2004;18(6):924-930. doipubmed
Jeon HW, Kim KS, Hyun KY, Park JK. Enucleation of giant esophageal schwannoma of the upper thoracic esophagus: reports of two cases. World J Surg Oncol. 2014;12:39. doipubmed
Shichinohe T, Kato K, Ebihara Y, Kurashima Y, Tsuchikawa T, Matsumoto J, Nakamura T, et al. Thoracoscopic enucleation of esophageal submucosal tumor by prone position under artificial pneumothorax by CO2 insufflation. Surg Laparosc Endosc Percutan Tech. 2014;24(2):e55-58. doipubmed
Makino T, Yamasaki M, Takeno A, Kurokawa Y, Miyata H, Takiguchi S, Nakajima K, et al. Thoracoscopic enucleation of esophageal schwannoma exhibiting (18) F-fluorodeoxyglucose uptake on positron emission tomography. Dis Esophagus. 2013;26(3):331-332. doipubmed
Liu T, Liu H, Yang C, Zhang X, Xu S, Liu B. Benign esophageal schwannoma compressing the trachea requiring esophagectomy: a case report. Thorac Cardiovasc Surg. 2013;61(6):505-506. doipubmed
Kitada M, Matsuda Y, Hayashi S, Ishibashi K, Oikawa K, Miyokawa N. Esophageal schwannoma: a case report. World J Surg Oncol. 2013;11:253. doipubmed
Kassis ES, Bansal S, Perrino C, Walker JP, Hitchcock C, Ross P, Jr., Daniel VC. Giant asymptomatic primary esophageal schwannoma. Ann Thorac Surg. 2012;93(4):e81-83. doipubmed
Wang S, Zheng J, Ruan Z, Huang H, Yang Z, Zheng J. Long-term survival in a rare case of malignant esophageal schwannoma cured by surgical excision. Ann Thorac Surg. 2011;92(1):357-358. doipubmed
Retrosi G, Nanni L, Ricci R, Manzoni C, Pintus C. Plexiform schwannoma of the esophagus in a child with neurofibromatosis type 2. J Pediatr Surg. 2009;44(7):1458-1461. doipubmed
Matsuki A, Kosugi S, Kanda T, Komukai S, Ohashi M, Umezu H, Mashima Y, et al. Schwannoma of the esophagus: a case exhibiting high 18F-fluorodeoxyglucose uptake in positron emission tomography imaging. Dis Esophagus. 2009;22(4):E6-E10. doipubmed
Zhang W, Xue X, Zhou Q. Benign esophageal schwannoma. South Med J. 2008;101(4):450-451. doipubmed
Yoon HY, Kim CB, Lee YH, Kim HG. An obstructing large schwannoma in the esophagus. J Gastrointest Surg. 2008;12(4):761-763. doipubmed
Mizuguchi S, Inoue K, Imagawa A, Kitano Y, Kameyama M, Ueda H, Inoue Y. Benign esophageal schwannoma compressing the trachea in pregnancy. Ann Thorac Surg. 2008;85(2):660-662. doipubmed
Tokunaga T, Takeda S, Sumimura J, Maeda H. Esophageal schwannoma: report of a case. Surg Today. 2007;37(6):500-502. doipubmed
Park BJ, Carrasquillo J, Bains MS, Flores RM. Giant benign esophageal schwannoma requiring esophagectomy. Ann Thorac Surg. 2006;82(1):340-342. doipubmed
Marin VP, Yu P, Weber RS. Isolated cervical esophageal reconstruction for rare esophageal tumors. Head Neck. 2006;28(9):856-860. doipubmed
Chen HC, Huang HJ, Wu CY, Lin TS, Fang HY. Esophageal schwannoma with tracheal compression. Thorac Cardiovasc Surg. 2006;54(8):555-558. doipubmed
Basoglu A, Celik B, Sengul TA, Yildiz L. Esophageal schwannoma. J Thorac Cardiovasc Surg. 2006;131(2):492-493. doipubmed
Dutta R, Kumar A, Jindal T, Tanveer N. Concurrent benign schwannoma of oesophagus and posterior mediastinum. Interact Cardiovasc Thorac Surg. 2009;9(6):1032-1034. doipubmed
Talbot M, Yee G, Saxena P. Endoscopic modalities for upper gastrointestinal leaks, fistulae and perforations. ANZ J Surg. 2017;87(3):171-176. doipubmed
This article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Medical Cases is published by Elmer Press Inc.